Saturday, 28 December 2024
PR. ANTHONY HILL - The UN Invents Climate Change and COVID-19 - What Now?


- https://muhammad-ali-ben-marcus.blogspot.com/2020/03/bill-gates-crown-corporations-and.html
Thursday, 19 March 2020
BILL GATES, THE CROWN, CORPORATIONS, AND GOVERNMENTS BEHIND THE CORONA SARS COV2 COVID19 VIRUS SCARE!

MY BLOG ATTACKED AS SOON AS I POSTED THIS, AND MY FACEBOOK ACCOUNT DE-ACTIVATED IN SEPTEMBER 2020!!!
DR. CHARLIE WARD ABOUT BILL GATES VACCINES DEATHS IN THE UK! ( A MUST WATCH!) (Sent to me today Wednesday 9 December 2020 by Barry Lyndon)
Dr. Charlie Ward
Коронавирус: маски вас не спасут :) / ЭПИДЕМИЯ с Антоном Красовским
13 Feb 2020
https://www.youtube.com/watch?v=FT4NWXTzhas&t=4s
Антон Красовски - ANTON KRASOVSKI
https://www.youtube.com/watch?v=9dUFZ3zSiXMDR. RASHID BUTTHAR[MURDERED LATER] BILL GATES, JACQUES ATTALI AND OTHER TOP JEWS HAVE BEEN PUSHING FOR THE EUGENICS AGENDA!
BILL GATES, JACQUES ATTALI AND OTHER TOP JEWS HAVE BEEN PUSHING FOR THE EUGENICS AGENDA!
Bill Gates annonce le programme : "Vacciner 7 milliards de personnes en bonne santé"55,208 views
•17 Apr 2020
163K subscribersBILL GATES WANT TO FORCE VACCINATE 7 BILLION PEOPLE!!!HE SHOULD BE ARRESTED AND DEPORTED TO ISRAEL!!!
Invité dans l’émission The Ellen Show présentée par Ellen DeGeneres du 13 avril 2020, le multimilliardiare philanthro-capitaliste Bill Gates, visiblement réjouit par la situation, a confirmé ses intentions : « Le vaccin changera la donne. »Une traduction ERTV. http://egaliteetreconciliation.fr/Bil...Pour soutenir ERTV : http://www.egaliteetreconciliation.fr...
THE WAR ON CHINA AND IRAN WITH ENGINEERED CORONAVIRUS SARS COV2 (COVID19) SCARE - FORT DIETRICH WHERE THE HIV VIRUS (?) AND HOAX WAS ENGINEERED!!!
https://www.youtube.com/watch?v=u4qdiY936gY
Tom Barnett's Coronavirus video
(removed by YT)
Ghost Town NYC – Is the Military conducting Clandestine Nocturnal Operations On Park Avenue in NYC?
JASON GOODMAN
It was French Zionist Jew Jacques Attali (ISRAEL) who called on live television for the TERMINATION of all old people ( above 65 or 70) who cost a lot to the State and nothing in return. The COVID-19 is a good test for that Jewish suggested EUTHANASIA Final Solution!
https://www.youtube.com/watch?v=b3bvOMBtDcE
Covid-19 : la solution ? Par Salim Laïbi
76K subscribers
Comme convenu, voici la vidéo qui revient sur toute l'actualité concernant l'épidémie de Coronavirus. Il s'agit de remettre cette analyse de l'épidémie dans son contexte plus large afin de mieux comprendre ce qui se passe. Il s'agit également de parler de la crise financière qui nous pendait au nez et qui sera camouflée par cette pandémie afin que les banksters puisse s'en tirer sans trop de casse. Lettre type pour les conflits d’intérêt : https://www.lelibrepenseur.org/covid-...Liens intéressants : - Vidéo Michel Cymès : https://www.facebook.com/watch/?v=889...Pour nous soutenir : - Tipeee : https://fr.tipeee.com/salim-laibi-le-... - Association de soutien : https://adsl.lelibrepenseur.org/Pour suivre nos travaux : - Facebook : https://www.facebook.com/LeLibrePense...- Notre site : https://www.lelibrepenseur.org- Se procurer nos livres : https://www.editionsfiatlux.com/
A COVER FOR 5G!!!While 359,000 citizens have been fined in France for not respecting the "CONFINEMENT" UKAZ, the UK is quickly installing 5G cables to KILL US!
https://www.youtube.com/watch?v=UDY5COg2P2c
ENGINEERED 1918 Spanish Swine Flu (KANSAS USA) historical documentary
Swine Flu Pandemic | Deadly plague of 1918
https://www.youtube.com/watch?v=UCGkd9hNbc046. COVID 19 - ISRAEL AS RULER OF THE MIDDLE EAST - CORONA
[Achtung! There are no such entities as "ISIS, Al Qaeda, Islamic Terrorist groups in the Sinai... Salafist Jihadis, Al Furqun Brigade, an Al Qaeda affiliate... " even if some Muslim fanatics have indeed joined them for purely personal, but not ISLAMIC reasons. All these and others have been proven hundreds of times to be CIA, NATO and MOSSAD mercenaries including MOSSAD agents posing as Muslims, debunked so many times!The world does not want to know, but SAUDIA in OCCUPIED ARABIA was created by the warmongering Western military powers with the complicity of the Khazarian Jews (KHAZAREL) and the entire decadent Christendom of the Synagogue of Satan at the end of WWI after they had defeated and dismantled the Ottoman Empire. Islam recognizes only ONE KING, GOD HIMSELF! Muslims are not Jews to have kings and kingdoms by the tons while living as minorities in Arabian-Egyptian-Persian lands.The original Saudis were Crypto-Jews from Basra and SAUDIA is ISRAILIYAAT! The Crypto-Jews called the Young Turks, from Salonika, were terrorists and mass murderers trained from Paris to infiltrate and overthrow the decadent Ottoman Caliphate, and they succeeded by mass-murdering Muslims and Christians alike - the much hated Amalekites by their bloodthirsty God of Israel! Zionist Crypto-Jew John Paul II hired a Jew LUSTIGER who converted to Catholicism at 14 (?) to take over the Catholic Church in France by making him Cardinal, Archbishop of Paris, and Chanoine! Lustiger himself admitted he was born a Jew, remained a Jew, and would die a Jew! Today, Christianity is dead in France, and they have replaced it with JUDEO-CHRISTIANITY subservient to the Apartheid entity known as ISRAEL!MARRANISME, SIONISME, LE JUIF CATHOLIQUE AARON - JEAN-MARIE LUSTIGER (1926-2007) Sunday, 20 November 2011
Saturday 28 March 2020
[BAFS]437 14 Share
3.72K subscribersCovid 19 is a fraud, but it's served its purpose.THAT was what 911 was about.
Expect a Fed crypto app - straight from The Fed to you. Maybe Trump will save the day? "Trust the plan"? :-D Understand The Belt & Road and Israel's central role, and it's move from "protectorate" seeking protectors, to a regional power. THAT was what 911 was about. This is what COVID 19 is about. This article lays it out for you: Bunting’s map and Israel on China’s new silk road - https://blogs.timesofisrael.com/bunti...Israel is getting ready to expand its borders. Covid 19 is a fraud, but it's served its purpose. We're distracted, in terror and not thinking. The "markers" in the virus have provided interesting data of transference mechanisms. Population movement is locked down - now for the real virus to wreak havoc? Or will it just blow over? Fabian Socialist style? We thought we were all gonna die! But they just wanted us in the right frame of mind for the Fed crypto app and a handout? Expect a Fed crypto app - straight from The Fed to you. Maybe Trump will save the day? "Trust the plan"? :-D Understand The Belt & Road and Israel's central role, and it's move from "protectorate" seeking protectors, to a regional power. THAT was what 911 was about. This is what COVID 19 is about. This article lays it out for you: Bunting’s map and Israel on China’s new silk road - https://blogs.timesofisrael.com/bunti...
MY BITCHUTE ACCOUNT: https://www.bitchute.com/channel/XfZS...
PATREON https://www.patreon.com/talpiot Acc Name: Brendon L. O'Connell Bank: St George Bank, Perth, Central Business District Acc No: 055164731 BSB: 116879 SWIFF Code: SGBLAU2S BTC - 12b5rUKgGBcnswh1JqsymvrzETvRGW5PND Bit Coin Cash - qpxtaj66vqnh4ra8g0nhu9kxy3267j7g5uu9nqgwz8 Ethereum - 0x21c6d2268806cb03579BD13A6d33f73DCb6Efc5B Litecoin - LYiHjTjzhC9RXZRWyznpG9UYyt2Frmn2LE
https://www.youtube.com/watch?v=jh1T4c3wP8I&feature=youtu.beDr Thomas Cowan : Virus et électrification de la Terre
1,709,844 views•16 Mar 2020Dr Wolfgang Wodarg on the current Corona pandemic
43,697 views•25 Mar 2020https://www.youtube.com/watch?v=0qwiyxedC_o
470 subscribersgepubliceerd als "How Dr. Wolfgang Wodarg sees the current Corona pandemic", https://youtu.be/p_AyuhbnPOI op "OVALmedia" op 13 maart 2020; https://www.youtube.com/channel/UCHFu...
https://www.youtube.com/watch?v=LJezTzLO5o8&t=186sTHE SCIENCE IS SETTLED!
And the survey says --CoronaMania is a HOAX!The Real History Channel surveyed 1,257 respondents (mostly Americans but also Europeans, Canadians and Australians)-- who in turn each know at least 30 people (conservative estimate) who in turn know at least another 25 other people. That gives us a random representative sample of almost 1 MILLION people within 2 degrees of separation of the original 1,257 survey respondents -- more than enough to make a truly SCIENTIFIC statistical extrapolation.
We asked just two questions:
1. Do you PERSONALLY know anyone who has died due to CV?
2. Do you PERSONALLY know anyone who PERSONALLY knows someone that has died due CV?
AMAZING RESULTS BELOW.*FINAL RESULTS
*Using very conservative numbers of relatives, neighbors, friends, co-workers, personal and online acquaintances etc.(Level 1 = 30 Contacts / Level 2 = 25 Contacts) -
March 28 - March 29 / Final
A - Number of Survey Respondents: 1,257B - Est. of acquaintances (1,257 x 30): 37,710C -Number of Deaths Personally Known: 3D -2nd Level Contacts (37,710 x 25): 942,750E- Deaths believed by 3rd Party Hearsay: 15* Final Tally (B+D):Out of 980,460 estimated extended contacts, only 18 (15 of which reported to us as hearsay!) -- know of (or think they know of ) a CV-related death -- with most comments indicating the deceased had other health problems or was over 70 years of age.Please Take our CoronaMania Survey
SURVEY CLOSEDThank you to all who participated.by Mike King*COMMENT FROM A READER"I don't know anyone who has died, but I do know of a few businesses that are dying."
*COMMENT FROM ANOTHER READER
"I KNOW OF ZERO CONTAMINATION CASES OR DEATHS, BUT I KNOW OF A PANDEMIC OF LIES BY THE USA, FRANCE AND BRITAIN ABOUT ITS CAUSES, TREATMENT, PROGNOSIS, BIG HARMA, AND SCAREMONGERING TACTICS, MEANING THEY WERE ALL HIDING SOMETHING OR PLANNING SOMETHING REALLY MONSTROUS AND DREADFUL (APOCALYPTIC)!!!!
BAFSCoronavirus : Actualité du 24 Mars 2020 - Mortalité, confinement, juridique, philo, bricolage...
DIGITAL I.D. WITH VACCINES, 5G, EUGENICS, TRANSGENDERARCHY, A.I.ARCHY, ETHNIC BOMBS, ... COMING TOO OR ALREADY HERE!!!
LE LIBREPENSEUR.ORGhttps://www.facebook.com/david.delaroque.1/videos/2692993597595531
ALMOST EXACTLY THE SAME AS COMMON COLD - SYMPTOM-WISE AND LESS LETHAL!
IT COULD BE A BIG PHARMA OPERATION WITH STATE COMPLICITY!
French Professeur Didier Raoult
WE KNOW HOW TO TREAT THE VIRUS!!!
https://muhammad-ali-ben-marcus.blogspot.com/2020/03/france-government-conspiracy-to-allow.html
FRANCE, GOVERNMENT CONSPIRACY TO ALLOW COVID 19 TO SPREAD. CUI BONO?

21st of January 2020 - on the Eugenics list of that 35 % at risk to die of COVID 19???My 2 grandchildren had both just had a course of antibiotics! After 4 consecutive days of high and intermittent fever and other seasonal and old age symptoms (kidneys, lungs, eyes, etc.,) I reported 7 of my symptoms I was more concerned with on 21st January 2020 to my "surgery", but the 'locum' doctor (my doctor went home because she had "the flu") refused to provide any medical help saying they had received instructions to CUT DOWN on prescriptions, including antibiotics, paracetamol, Gaviscon, etc.! She was not even willing to listen to me, and when I objected, she said I can buy medication over the counter, but she finally prescribed me Gaviscon (anti-acid)?When I complained about the 'locum' or 'locust doctor' at the reception and asked to be seen by my regular doctor, a very unsympathetic elderly (?) lady was very unpleasant and said the 'locum' was right and stressed that I was registered to the surgery and not to a particular doctor. As I can heal acidity by myself, I did not take the prescription to the HARMacy (BIG HARMA!)! And, I did not return to the "surgery" since that day but tried my best to take care of myself without medical help - and I am 74 years old and living alone!I immediately suspected that the Government was into a huge scam regarding health care as well as in a conspiracy to make Corporations make more profits as I saw on the counter and in supermarkets medication being offered at twice or thrice the usual price! 21 OCTOBER 2010 - 12:14-12:26
21 OCTOBER 2010 - 12:14-12:26
[A YEAR AFTER THE 2009 FAKE SWINE FLU H1N1 PANDEMIC]
Outbreak timeline2009 UK swine flu outbreak, milestone 27 April First two UK H1N1 cases confirmed in Scotland after a flight from Mexico.[17] 29 April Paignton Community and Sports College closes for about a week in first school closure.[18] 1 May First two UK person to person transmissions confirmed.[19] 2 May Further schools are temporarily closed from this date.[20][21][22][23] 7 May HPA issues advice on exclusion from schools and workplaces.[24] 8 May HPA issues "advice on actions to be taken in a school in the event of a probable or confirmed case of "swine flu" being identified in a school pupil",[25] in which closure for 7 days is advised when appropriate. The virus from European samples isolated and its full genetic fingerprint determined by UK researchers,[26] following similar work in the US on the virus in the American continent. 17 May One hundredth confirmed case.[27] 22 May HPA staff no longer routinely meet flights from Mexico. Contact tracing of passengers deemed to be at risk of swine flu carried out on the basis of risk, as for other communicable diseases.[28] 26 May The largest single outbreak so far, with 50[29] confirmed cases identified at a Birmingham primary school (later increased to 74[30]). 13 June Over 1,000 cases of swine flu confirmed in the UK.[2] 14 June First death, of patient with underlying health problems, reported at the Royal Alexandra Hospital in Paisley, Glasgow, Scotland.[31] 26 June Second death, of patient with underlying health problems, of a six-year-old girl at Birmingham Children's Hospital in the West Midlands region. Her death was reported on 29 June.[32] 30 June 6,000 cases of swine flu confirmed in the UK.[33] 2 July The HPA announced that the containment approach to reduce spread was no longer appropriate given the clusters of cases around the UK, and would be replaced by a treatment phase in which everybody presenting symptoms would be treated if necessary without laboratory confirmation, but contacts would not be traced. Daily reports of confirmed cases are no longer being published.[34] 6 July Three deaths in the UK bringing the total to seven. The new victims include two 9-year-old girls. NHS stated all three had "serious underlying health problems". The victims are from South London and Dewsbury in West Yorkshire.[35] 9 July The government announced that there are now over 9,000 cases of Swine flu in the UK and 14 patients have died,[36] 2 in Scotland, 5 in London, and the remainder elsewhere in England.[37] 10 July A 15th person has died from swine flu in Essex. Unlike previous cases, they had no underlying health conditions.[38] 13 July 2 more people die with swine flu in England.[39] One, a 6-year-old girl, who died of septacemia, and a middle-aged doctor. Initial reports that he died of Pulmonary Embolism were disproved on his final Post Mortem, which concluded that Swine Flu was a contributing factor in his death.[40] 16 July It emerges that 12 more people have died. The total now stands at 29. 85,000 people are estimated to be affected by swine flu as of 16 July, with 55,000 new infections in the preceding week according to HPA modelling.[41] 23 July The National Pandemic Flu Service goes live in England for the first time.[42] Shortly after it goes live, the Service gets over 2,000 hits per second. Scotland, Wales and Northern Ireland can opt in for the service if the rate of infection increases. 21 August The first swine flu related death in Wales has been confirmed after a 55-year-old woman died.[43] 15 October Its announced that there were 27,000 new swine flu cases in the past week, up from 18,000 the week before, and new cases were rising more slowly than expected, but the number requiring treatment in intensive care had increased from 47 out of 290 hospitalised last week to 74 out of 364 hospitalised this week. The number of deaths in the UK rose to 106.[44] 21 October Swine Flu Vaccine became available across the UK and mass immunisation programme gets under way.[45] 22 October It's announced that Swine flu cases in the UK almost doubled from the previous week to 53,000. The number of patients needing hospital care has risen to 506 in England with 99 in critical care – the highest since the pandemic began. Deaths increased to 128. The total number of cases is now estimated to be 435,000.[46] 29 October Swine Flu cases rose by almost 50% to 78,000 new cases. Deaths increased to 137. Hospitalised patients increased to 751, of which 157 are in intensive care including nine people on ECMO (extracorporeal membrane oxygenation) machines. It is now estimated that there have been 521,000 cases in England since the pandemic began. It is also reported that one in three deaths are not in the "priority vaccination group" as currently defined by the government.[47] 5 November New Swine Flu cases increased to 84,000. Deaths increased to 154. 848 people are hospitalised, 172 of which are in intensive care. It is thought that the rise in new cases was smaller this week due to school children being on their "half term" holidays. Andrew Lansley, the Shadow Health Secretary, called on the Government to commit to vaccinating all schoolchildren in the country, as well as university students.[48] 12 November The number of new swine flu cases in the past week fell by nearly a quarter to 64,000 in England. Deaths increased to 182 (124 deaths in England, 33 in Scotland, 11 in Northern Ireland and 14 in Wales).[49] Hospitalised patients fell to 785, of whom 173 are in intensive care. The Chief Medical Officer, Sir Liam Donaldson, said that the drop in new cases could be due to school children's half term break, the impact of which could last two weeks and that next week's figures should give a clearer picture of how the virus is developing. Shadow health secretary Andrew Lansley said the latest figures again illustrated the importance of vaccinating children. "This is further evidence that we need to begin planning a school and college-based vaccination programme immediately."[50][51] 19 November New Swine Flu cases decreased again from the previous week, down to 53,000 new cases in England in the last week. 783 patients were hospitalised. The number of deaths related to swine flu in the UK increased to 214[52] (142 in England). The HPA estimates that there have now been a total of 715,000 cases of swine flu since the pandemic began.[53][54] The government has announced that all children under the age of five are to get the swine flu vaccine. Chief Medical Officer Sir Liam Donaldson said there had been a rise in serious illnesses recently among young children that was "causing concern". "We consider them to be seriously at risk". Latest figures showed that 81% of under-5s hospitalised with swine flu had no underlying health issues. The Conservative Party says that all under-25s should get the vaccine next.[49][55] 20 November The first officially confirmed cases of person-to-person transmission of a Tamiflu-resistant strain of swine flu in the world are reported to have happened between 5 patients at the University Hospital of Wales in Cardiff.[56] 26 November The number of new swine flu cases continue to fall, with 46,000 new cases in the last week, 7,000 less than the week before. However Swine flu deaths in England in a single week reached their highest level with a record 21 deaths, bringing the total deaths to 245 in the UK (163 in England). There were 753 hospitalised patients, 154 of those being in intensive care. The Government estimates more than a million people have now been vaccinated, roughly a month after the vaccination program started (that figure excludes health care workers, who are also being offered the vaccine). That means only about 1 in 10 of the 11 million people in the "at risk" priority groups have so far been vaccinated. Professor David Salisbury, head of immunisation at the Department of Health was disappointed, saying "Clearly I would have liked a bigger number...I would like to see an acceleration now".[57][58] 3 December New Swine Flu cases more than halved from the previous week, dropping to 22,000 new cases in England in the last week. Total deaths increased to 270 (178 deaths in England). There are 747 hospitalised patients – 161 of which are in critical care. A further 600,000 people were vaccinated in the last week, bringing total to 1.6 million people. In addition to that, 275,000 healthcare workers have been vaccinated out of nearly 2 million. Chief Medical Officer Sir Liam Donaldson said it was still "too early" to know whether the downward trend in new cases would continue and that his biggest worry was the virus mutating or mixing with other viruses and creating a new, more dangerous virus. Prof David Salisbury, head of immunisation at the Department of Health, said the vaccines with adjuvants, substances which boost the immune system and allow less active ingredient to be used in each dose, offer good protection even if the virus does change; "One of the advantages with adjuvanted vaccines is their ability to protect against drifted (mutated) strains. It opens the door for a whole new strategy in dealing with flu." The GlaxoSmithKline vaccine, Pandemrix, which forms the bulk of the governments mass vaccination programme with 11.2 million doses delivered so far to health services, contains an adjuvant.[59][60][61][62] 10 December New Swine Flu cases halved from the previous week, to 11,000 new cases in England. Deaths increased to 283 (191 in England) and there were currently 636 hospitalised patients. The number of people vaccinated increased to 2.3 million. The estimated total number of cases is 795,000. The Chief Medical Officer Sir Liam Donaldson revealed that the swine flu pandemic is "considerably less lethal" than feared. An analysis of deaths to 8 November showed that 26 people have died for every 100,000 cases in England, meaning a death rate of 0.026% in those infected with Swine Flu. The highest death rate was in those aged over 65, and lowest in those aged 5 to 14. The average age at death was 39. Of the patients who died, 67% were in the "high risk" vaccination priority group and were eligible to get vaccinated, 36% had either no or only mild pre-existing illnesses. Sir Liam again urged people to come forward for immunisation, commenting that a lower impact than previously feared "is not a justification for public health inaction. Our data supports the priority vaccination of high risk groups. Given that a substantial minority of deaths occur in previously healthy people, there is a case for extending the vaccination programme".[63][64][65][66] 17 December New Swine Flu cases again fell with 9000 people infected in last week. Total deaths in the UK increased to 299 (203 in England). The number of currently hospitalised patients fell to 523 patients of which more than 100 were in intensive care. 3 million people out of the 9 million in the 1st vaccination priority groups have now been vaccinated including 100,000 pregnant women. In addition to that, 343,000 front line health workers have also been vaccinated. It appears that the second wave of Swine Flu is coming to an end but experts warn cases could rise again in the future in a "third wave" of swine flu.[67][68][69][70][71] 24 December New cases of Swine Flu fell by a third to 6,000 cases this week. The total death figures will be updated by the HPA on Thursday 7 January. The number of hospitalised patients declined to 454 currently in hospital (as of 8 am on 23 December).[72] 31 December The HPA did not release estimate numbers this week, instead saying that flu activity is continuing to decrease across the UK but some caution must be exercised as this may be influenced by the holiday period. 496 patients were currently hospitalised in England as of 8 am on 30 December (an increase from last week). A more detailed update will be released next week.[73] 8 January Swine Flu cases continued to decrease, down to less than 5,000 new cases in the preceding week. Total UK deaths increased to 360 (251 in England, 64 in Scotland, 28 in Wales and 17 in Northern Ireland). Hospitalised patients in England (as of 8 am on 6 January) numbered 393, of whom 103 were in critical care. Only 3.2 million people had been vaccinated (out of 9 million in the priority groups), including 113,000 pregnant women (out of roughly 600,000), 86,000 under-5s (out of more than 3 million) and an additional 373,000 front-line health workers (out of more than a million). The Head of Immunisation at the Department of Health, Professor David Salisbury urged all those in the at-risk priority groups to get immunised, especially children under five and those with underlying health conditions, because while cases were currently down, it was not clear what would happen with swine flu over the year ahead.[74][75][76]
 21 OCTOBER 2010 - 12:14-12:26
21 OCTOBER 2010 - 12:14-12:26 21 OCTOBER 2010 - 12:14-12:26
21 OCTOBER 2010 - 12:14-12:26 21 OCTOBER 2010 - 12:14-12:26
21 OCTOBER 2010 - 12:14-12:26
21 OCTOBER 2010 - 12:14-12:26
I suspected such a scam the same day I photographed for the very first-time EXTREMELY UNUSUAL CHEMTRAILS over our house and informed the sheeple on the Internet that same day. After the government had announced a 2nd wave of the BOGUS SWINE FLU epidemic in the next winter season where the media printed such lies that we should expect 60,000 dead the following season and burial in communal graves! The media are all owned by the same Corporations!
MUAMMAR AL GHADDAFI:
The West contaminates the world with viruses FOR PROFITS!
He added that vaccines and medicine must not be sold or BE FREE!
A PARTAGER UN MAXIMUM SVP
LISEZ BIEN MERCI
[ALERTE CHLOROQUINE]
Chers amis, j'aimerais vraiment vous sensibiliser sur ce sujet très important de la Chloroquine et j'aimerais vraiment que vous preniez le temps de lire ces quelques lignes.
Car ce qu'il se passe actuellement autour de ce médicament est très révélateur et va nous inviter très prochainement à être très très prudent.
Tout lien reflétant mes propos est en bas de page. Vos avis, remarques ou critiques sont évidemment les bienvenus.
Petit rappel des faits pour bien comprendre :
Le 25 février 2020, le Docteur Raoult, infectiologue Français réputé à l'IHU de Marseille, en collaboration avec les experts chinois, signalait dans une vidéo avoir eu d'excellent résultat avec un médicament très connu du monde médical : La chloroquine. Ce médicament, antipaludique, existe depuis plusieurs dizaines d'années et serait très efficace contre le COVID-19. Très efficace au point que sur 24 patients infectés par le coronavirus à Marseille, trois quarts d'entres eux n'étaient plus porteurs du virus, après seulement 6 jours !! Oui, 6 jours !!
Un succès attribué à la combinaison de la chloroquine avec une autre substance active, l’azithromycine.
Cet antipaludique serait donc en mesure de soigner les plus sévèrement touchés et pourrait permettre de faire baisser drastiquement l'évolution épidémique en France.
Nous avons donc un médicament, immédiatement disponible et très peu coûteux, qui pourrait sauver des milliers de vies mais en France, on préfère essayer d'autres méthodes, totalement inefficaces avec les moyens qu'on lui donne, comme le confinement général du pays ! Avec toutes les conséquences que cela aura sur notre économie toute entière. Toutes ces faillites d'entreprises à venir, tous ces gens au chomage. C'est juste hallucinant et totalement irresponsable !!
La suite est encore plus hallucinante :
Qu'a t-on appris récemment ?
D'une part que ce docteur Raoult subit depuis plusieurs semaines des menaces pour qu'il retire ses propos. Des menaces qui auront quand même poussé le docteur à porter plainte.
Que Agnès BUZIN, ex ministre de la santé, qui après avoir laissé sciemment le virus se répandre sur tout le territoire avec l'aide de Philippe et Macron, en laissant les frontières ouvertes, sans aucun contrôle aux aéroport ni confinement des français rapatriés, aurait classé la Chloroquine, médicament jusqu'ici délivré sans ordonnance, comme substance vénéneuse, et ce dès Janvier 2020 ! Soit quelques jours avant le début de l'épidémie. Oui la chloroquine est désormais interdite en vente libre !
EDIT :
08 octobre 2019 : L'ANMS saisit l'ANSES pour l'interdiction de l’hydroxychloroquine
12 Novembre 2019 : L'ANSES donne son accord.
Décembre 2019 : Début épidémie en Chine.
13 janvier 2020 : Mis en vigueur de l'interdiction par arrêté.
24 janvier 2020 : 1er cas de coronavirus en France.
Pourtant dans le monde, tout s'accélère et un incroyable retournement de situation est en train de se faire.
Car après que la Chine ai décidé d'utiliser ce traitement et qui je le rappelle, est sortie de crise, c'est au tour de Donald Trump, président des États Unis, de décider de valider le produit et de lancer une production à grande échelle sur tout le sol américain de ce médicament ! Le Maroc à lui aussi hier, acheter tout un stock de Chloroquine à Sanofi !
On attend quoi en France avec la vague mortelle qui arrive ?? Regardez l'Italie, dans 6 jours on est comme eux !Avec des hôpitaux qui sont déjà au bord de la rupture !
La suite est pour moi encore plus hallucinante :
Nous apprenons hier, par le Pr Christian Perronne, chef de service en infectiologie à l’hôpital de Garches, que tout notre stock de Chloroquine, qui aurait pu servir à sauver des milliers de vie je le rappelle, que tout ce stock a été, volé cette nuit !!!
Oui vous avez bien lu, on s'est fait "volé" tout un stock de chloroquine avec des milliers de doses, dans un entrepôt national, des tonnes de produit, comme ca, d'un coup, en une nuit !
Par qui, on se demande !! Qui peut faire une chose pareille et surtout qui en a les moyens logistique ??
Mettons les thèses complotistes de côté, il ne s'agit pas de fantasmes, mais bien de réalité !
Très honnêtement, entre cette problématique de chloroquine prometteuse indisponible, interdite et maintenant volée. Cette impossibilité de s'équiper en test de diagnostic comme l'on fait les coréens qui sont eux aussi déjà sortis de la crise. Cette pseudo pénurie de gants, de gels et de masques pour nous protéger, dans les pharmacies, dans les hôpitaux et sur tout le territoire français. Vous pensez que c'est une affaire de moyen? Que nous sommes un pays sous développé ??
PUTAIN, LA FRANCE, 7ÈME PUISSANCE MONDIALE !!
Ne trouvez vous pas que quelque chose cloche/choque ?
Si tout est normal pour vous, rendormez vous. Les autres, je vous invite à vous méfier très fortement, pour prendre le moment venu toutes les dispositions nécessaires à votre maintien en sécurité.
Non, Macron ne nous sauvera pas de la catastrophe en cours, bien au contraire. Ce n'est pas son objectif, ni celui de ceux qui l'ont mis au pouvoir.
Car au delà de l'épidémie sur laquelle tout le monde se focalise, il y a un autre très gros problème dont on parle très peu et qui fera selon moi bien plus de victimes, c'est l'effondrement de l'économie mondiale en cours et de ces milliers de milliards que les banques centrales injectent depuis plusieurs semaines pour soutenir un système qui s'écroule. Les conséquences vont être dramatiques en termes de faillites et chômage de masse. Et n'allez pas me dire que nos élites l'ignorent.
Bref, si je devais donner un conseil, c'est de rester informé, car un public non informé réagit comme "programme".
Coronavirus:Chloroquine, fin de partie
https://www.youtube.com/watch?v=8L6ehRif-v8
Menace sur le docteur
https://video-cdt1-1.xx.fbcdn.net/v/t42.9040-2/90314139_905931319844648_8292635555611541504_n.mp4?_nc_cat=103&_nc_sid=985c63&efg=eyJ2ZW5jb2RlX3RhZyI6InN2ZV9zZCJ9&_nc_ohc=tRXEumY4ar0AX9HbQ6z&_nc_ht=video-cdt1-1.xx&oh=1a39fdc86145ec3dcfa0225012d3050e&oe=5E76C165
Chloroquine sur liste vénéneuse
https://www.egaliteetreconciliation.fr/Agnes-Buzyn-a-t-elle-fait-classer-la-chloroquine-en-substance-veneneuse-le-13-janvier-2020-58593.html
Buzin savait :
https://www.upr.fr/actualite/une-bombe-politique-agnes-buzyn-soulage-sa-conscience-dans-le-journal-le-monde-et-accuse-implicitement-macron-detre-responsable-de-milliers-de-morts-a-venir/
Vol des stocks de Chloroquine :
https://www.ndf.fr/politique/21-03-2020/ce-nest-pas-une-blague-nos-stocks-de-chloroquine-possible-remede-contre-le-covid-19-auraient-ete-voles-selon-le-pr-christian-perronne-chef-de-service-en-infectiologie-a-lhopital-de-garche/
TRUMP
https://www.marianne.net/politique/de-marseille-fox-news-comment-les-essais-de-didier-raoult-sur-la-chloroquine-ont-convaincu
MAROC
https://www.francetvinfo.fr/monde/afrique/societe-africaine/covid-19-le-maroc-achete-les-stocks-de-nivaquine-produits-par-sanofi-dans-une-usine-de-casablanca_3876461.html
lien de l'étude prépubliée par l'équipe du Pr Didier #Raoult :
https://lelibrepenseur.org/wp-content/uploads/2020/03/covid-19-hydroxychloroquine-and-azithromycin-as-a-treatment-of-covid-19.pdf
Arrêté du 13 janvier 2020 portant classement sur les listes des substances vénéneuses
https://www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000041400024&categorieLien=id See Less
https://www.youtube.com/watch?v=DrmT0XNpZyACoronavirus : Actualité du 23 Mars 2020 - Tests, Pr Raoult, effets secondaires, témoignages...
Comme convenu, voici le 4e numéro de l'actualité concernant l'épidémie de Coronavirus que nous tenons à jour quotidiennement et en direct à 20 heures 05 afin de réparer la désinformation des médias mainstream.
https://www.youtube.com/watch?v=9QQNItLLki0
Coronavirus : tests publics gratuits à Marseille
2.2K 45 Share
64.9K subscribers
En direct de Marseille, de l'hôpital de la Timone dans le service du professeur Didier Raoult des maladies infectieuses, vous pouvez constater que les tests à grande échelle du Coronavirus sont pratiqués gratuitement sur tous ceux qui veulent les faire, avec ou sans symptomatologie. Si le test s'avère positif, il vous sera proposé le traitement à l'hydroxychloroquine + azithromycine comme expliqué par le professeur Didier Raoult. Bizarrement, absolument aucun média officiel ne parle de cette initiative essentielle à l'éradication de l'épidémie. Pourtant, de nombreux hôpitaux français proposent aujourd'hui comme traitement aux patients atteints du Civid-19 hydroxychloroquine et l'azithromycine ! On marche sur la tête en France et ce sont les médias qui autorisent ou non des protocoles médicaux !!!
https://www.youtube.com/watch?v=Itaw7HWxTXcCoronavirus : actualité du 21 Mars 2020
578 8 Share Save
64.9K subscribers
Ils assistent à l’enterrement de leur proche et se voient verbalisés pour non-respect du confinement 23/03/2020

Quatre personnes ont été arrêtées par les gendarmes puis verbalisées à Falaise, dans le Calvados, pour «non-respect des règles de confinement» après avoir assisté à l’enterrement d’une de leurs proches.
Les gendarmes ont arrêté quatre personnes qui rentraient chez elles en voiture après avoir enterré leur proche au cimetière de Guibray, à Falaise dans le Calvados, rapporte Ouest-France.
Après vérification de leurs attestations de déplacement, deux gendarmes décident de les verbaliser pour «non-respect des règles du confinement». «C’est complètement aberrant», dénonce Benjamin Loison, petit-fils de la défunte.
«Pour la mise en bière, nous sommes entrés un par un dans la pièce. Lors de la cérémonie, nous étions bien tous à plus d’un mètre les uns des autres. Nous étions 15 personnes, ce qui était le maximum autorisé», raconte-t-il.
Pas de «motif valable»
Selon M.Loison, les proches de la défunte détenaient «l’acte de décès en plus de l’attestation de déplacement dérogatoire», mais le gendarme leur a dit que «ce n’était pas un motif valable» en pleine pandémie de nouveau coronavirus.
«La personne des pompes funèbres s’est même déplacée pour venir lui confirmer qu’on sortait de l’enterrement. Mais il n’a rien voulu entendre», déplore-t-il.
La famille a fini par contacter la mairie de Falaise ainsi que la préfecture du Calvados, qui ont estimé, d’après M.Loison, qu’il n’y avait pas lieu de les verbaliser.
https://fr.sputniknews.com/france/202003221043355634-ils-assistent-a-lenterrement-de-leur-proche-et-se-voient-verbalises-pour-non-respect-du-confinement/
Viruses (WIKIPEDIA)
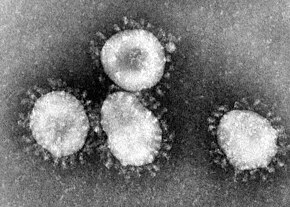 The common cold is a viral infection of the upper respiratory tract. The most commonly implicated virus is a rhinovirus (30–80%), a type of picornavirus with 99 known serotypes.[29][30] Other commonly implicated viruses include human coronavirus (≈ 15%),[31][32] influenza viruses (10–15%),[33] adenoviruses (5%),[33] human respiratory syncytial virus (orthopneumovirus), enteroviruses other than rhinoviruses, human parainfluenza viruses, and human metapneumovirus.[34] Frequently more than one virus is present.[35] In total, more than 200 viral types are associated with colds.[3]Coronaviruses are a group of viruses known for causing the common cold. They have a halo or crown-like (corona) appearance when viewed under an electron microscope.
The common cold is a viral infection of the upper respiratory tract. The most commonly implicated virus is a rhinovirus (30–80%), a type of picornavirus with 99 known serotypes.[29][30] Other commonly implicated viruses include human coronavirus (≈ 15%),[31][32] influenza viruses (10–15%),[33] adenoviruses (5%),[33] human respiratory syncytial virus (orthopneumovirus), enteroviruses other than rhinoviruses, human parainfluenza viruses, and human metapneumovirus.[34] Frequently more than one virus is present.[35] In total, more than 200 viral types are associated with colds.[3]Coronaviruses are a group of viruses known for causing the common cold. They have a halo or crown-like (corona) appearance when viewed under an electron microscope.
- Pelczar (2010). Microbiology: Application Based Approach. p. 656. ISBN 978-0-07-015147-5. Archived from the original on 16 May 2016.
* TRUMP LIED ABOUT HIS 8 BILLION DOLLARS AND* MACRON LIED ABOUT HIS 150 BILLON EUROSTHEY SAID THEY WILL INVEST TO FIND VACCINES AND THERAPEUTIC TREATMENTS FOR THE CORONA VIRUS!WHEN THE TREATMENT ALREADY EXISTS???*BORIS IS OFFERING £330 BILLION PACK LOANS TO WHOM??? AND FOR WHAT???ZERO FRESH BREAD +ZERO SLICED BREAD +ZERO HYGIENIC PAPER +ZERO MILK +ZERO PASTA +
DEADLIER THAN THE CORONAVIRUS!!!
+ BRITISH 'CITIZENS' (SUBJECTS) FIGHTING, SCREAMING, SWEARING, LITERALLY BEHAVING LIKE WILD ANIMALS!!! +
+ CUSTOMER HYSTERIA AND VIOLENCE
+ CONFINEMENT =PROOF OF GOVERNMENT STAGED PANIC FOR ECONOMIC AND POLICE TOTALITARIAN STATE REASONS!
CORONAVIRUS - ON SAIT GUÉRIR LA MALADIE Dixit le professeur Didier Raoult
https://www.youtube.com/watch?v=tQ2Elyy-xRc&t=315s
Dieudonné : Chloroquine
11,368 views•Premiered 2 hours ago - Lundi 23 mars 2020WE KNOW HOW TO TREAT CORONAVIRUS COVID19!!! THE SAME TREATMENT AS FOR MALARIA!!! (PALUDISME)
2,450 views•19 Mar 2020https://www.youtube.com/watch?v=32t7Uif9Twg
32.5K subscribers
Le test clinique réalisé sur 24 patients de l’IHU de Marseille avec de l’hydroxychloroquine serait efficace contre le coronavirus selon des premiers résultats présentés par le professeur Raoult🎯 J’ai mis en place l’Uppercut pour mes contacts privés, j’envoie chaque matin ta dose quotidienne de motivation sans filtre : https://goo.gl/PWEPxv
https://www.youtube.com/watch?v=4wRAr16GvUIActu au Scalpel 63 : Coronavirus, ce que les médias vous cachent
59,337 views•Premiered on 29 Feb 2020
57.2K subscribers
Cet épisode 63 de l'Actu au Scalpel revient sur l'affaire du coronavirus. Il sera question ici aussi bien de l'épidémie que du traitement médiatique assez lamentable de cette affaire. On reviendra également sur certains points de l'histoire qui vont nous aider à mieux comprendre ce qui se passe.Pour nous soutenir : - Association de soutien : https://adsl.lelibrepenseur.org/- Tipeee : https://fr.tipeee.com/salim-laibi-le-...Pour suivre nos travaux :- Notre site : https://www.lelibrepenseur.org/- Se procurer nos livres : https://www.editionsfiatlux.com/
https://www.youtube.com/watch?v=TADna6HNsRk
MARSEILLE
Coronavirus : Actualités du 20 mars 2020 - Urgences dentaires
14,256 views•Streamed live 4 hours ago
64.3K subscribers
Nous allons réaliser tous les soirs à 20h une vidéo pour traiter de l'actualité du #coronavirus en France et dans le monde. Ceci vous fera rater le journal de désinformation du 20h et fera baisser le stress ambiant, ce qui ne peut être que bénéfique pour votre organisme :) Il s'agit dans ce numéro de vous parler du traitement des urgences dentaires depuis la mise en place du confinement. Comment faire, qui appeler lorsque l'on se retrouve dans certaines situations. Vous pouvez posez vos questions dans les commentaires, on y répondra dès que possible. Merci de partager au plus grand nombre. :)
https://www.youtube.com/watch?v=h-cAeQGpNq8Coronavirus : Actualité du 27 Mars 2020 - Propagande, Effets secondaires du Kaletra, Crise finance...
 MIKA MIKAZE IN REUNION ISLAND
MIKA MIKAZE IN REUNION ISLAND
L’ambassade de Chine en France suggère à son tour une origine américaine de la COVID-19 23/03/2020
 HASHEM EFFACERA JUSQU'AU SOUVENIR D'AMALEK!
HASHEM EFFACERA JUSQU'AU SOUVENIR D'AMALEK!
L’ambassade de Chine en France a suggéré lundi dans une série de tweets que la pandémie de COVID-19 avait débuté aux États-Unis, reprenant des accusations chinoises contre les Américains sur l’origine du coronavirus qui s’est d’abord répandu sur une grande échelle en Chine.
« Combien de cas de COVID-19 y avait-il parmi les 20 000 morts de la grippe qui a commencé en septembre dernier ? », se demande-t-elle dans une série d’interrogations en forme d’affirmations, sans éléments scientifiques à l’appui.
Les États-Unis n’ont-ils « pas tenté de dissimuler la pneumonie du nouveau coronavirus par la grippe ? », poursuit-elle sur Twitter, un réseau social par ailleurs bloqué en Chine et où circulent de très nombreuses fausses informations, rumeurs et manipulations sur la COVID-19.
Pékin et Washington sont engagés dans une guerre des mots et désormais de l’information sur l’origine de la pandémie, Donald Trump parlant de « virus chinois » depuis son apparition en décembre en Chine, au grand dam des autorités chinoises.
Un porte-parole du ministère chinois des Affaires étrangères, Zhao Lijian, avait déjà laissé entendre le 13 mars que l’armée américaine avait introduit le virus à Wuhan, la ville de Chine d’où est partie l’épidémie selon la plupart des scientifiques, au cours des Jeux mondiaux militaires d’octobre.
Les États-Unis ont pour leur part accusé la Chine de semer des « rumeurs abracadabrantes » sur l’origine du coronavirus et de « propager des théories du complot » relayées sur les réseaux sociaux.
L’ambassade de Chine fait désormais ouvertement le lien avec la « fermeture surprise en juillet dernier du plus grand centre de recherche américain d’armes biochimiques, la base de Fort Detrick au Maryland ».
« Après la fermeture, une série de cas de pneumonie ou des cas similaires (sont) apparus aux États-Unis », affirme-t-elle, reprenant à son compte des supputations qui circulent sur l’internet.
Elle laisse aussi entendre que le virus était présent dès la fin 2019 en Italie et que la plupart des premiers cas détectés en Australie provenaient des États-Unis.
https://www.lapresse.ca/international/europe/202003/23/01-5265983-lambassade-de-chine-en-france-suggere-a-son-tour-une-origine-americaine-de-la-covid-19.phpCoronavirus : Le bilan tragique au stade 3 : "MALHEUR À TOI, PAYS DONT LE ROI EST UN ENFANT !"
FRANÇOIS ASSELINEAU
318,217 views•17 Mar 2020https://www.youtube.com/watch?v=HlMXnKJhqfA&t=1679s
 MIKA
MIKA
https://www.youtube.com/watch?v=L8YDw3RSy7A
Traitement contre le Coronavirus : Didier Raoult estime que la chloroquine est "susceptible d'êtr…
62,317 views•26 Feb 2020
481K subscribersFace à l'épidémie grandissante de Coronavirus qui sévit désormais en Europe avec 10 morts en Italie et deux nouveaux cas détectés en France, des chercheurs auraient trouvé un traitement contre le paludisme qui pourrait traiter le virus. Pour en parler, Matthieu Belliard reçoit Didier Raoult, infectiologue au Pôle de maladies infectieuses au CHU de la Timone à Marseille et directeur de l'Institut Méditerranée Infection à Marseille.
https://www.youtube.com/watch?v=lnbVg_fGM0k
Interview du Professeur Didier Raoult
25,740 views•21 Feb 2020L’épidémie du nouveau coronavirus s'est déclarée il y a près d'un mois. A cet effet, le gouvernement chinois a pris une série de mesures, validées par des spécialistes étrangers du secteur médical. Notre correspondante Michelle Ma a interviewé M. Didier Raoult, professeur de microbiologie à l’Université Aix-Marseille en France. Voici le reportage. Sélection des meilleurs reportages de la rédaction du " Journal " de CGTN Français.BILL GATES AND HIS DEADLY VACCINES KICKED OUT OF INDIA!
https://www.youtube.com/watch?v=Q5rBrjs32kI
JASON GOODMAN
Ghost Town NYC – Is the NY Post Threatening Jason Goodman & Charles Ortel with Another #FakeBombPlot
102K subscribers
The New York Post published a story about an alleged bomb plot against the very statute Charles Ortel and I visited on Sunday. As ridiculous as it sounds to bomb an inconsequentially bronze statue, could this story be true or is it a veiled threat against Jason & Charles? Become a Sponsor of Crowdsource the Truth & enjoy exclusive content on SubscribeStar & Patreon
BILL GATES - PIE IN FACE Belgium, circa 1999!
DOCTORS ARE ALREADY PRESCRIBING TONS OF KILLING MEDICATION TO PROFIT BIG PHARMA WITH STATE COMPLICITY!
Bill Gates Talks about Coronavirus-Like Epidemic in 2019 Netflix Documentary
Updated on Jan 31, 2020 at 8:11 am UTC by Teuta Franjkovic · 4 min read
In November Netflix released a documentary about the coronavirus-like epidemic and Bill Gates spoke there like a real Nostradamus. He said we should invest more in the development of vaccines against such diseases.When last year in November, a documentary series episode from Netflix called “The Next Pandemic” came out – nobody actually didn’t give it too much importance. However, only a month after – boy, how it started to be popular. The episode describes the ways how viruses are spreading and evolving into epidemic situations.
The story starts with traveling across India, Egypt, the Democratic Republic of Congo, the United States and explains historical cases of pandemics like it was the Spanish flu of 1918 or Ebola and the bird flu.
Chinese Wet Markets are Batch of Disease
The point is that the documentary says that in wet markets in China, people are trading with various live animals who are then being slaughtered on sight by vendors who then sell meat to consumers.
And, just to explain a bit. The author of this article has been traveling through Asia a lot. And I love food. And I’ve seen wet markets in Hong Kong, Singapore, Bali, Taiwan – and they are all pretty normal and decent. Maybe a little bit dirtier because of the climate there, but nothing special. But I couldn’t go to mainland China wet markets. Wushu, Shenzhen and even Shanghai seem to be another culture.
In Humid Conditions the Virus Evolves
From eating pigeons and dogs and rats and lizards and bats – to not giving a damn about any hygiene, not to talk about any humanity when killing those animals at the spot. So yes. When Netflix describes the wet markets as a disease X factory – they couldn’t be more right. When you have such conditions (humidity, dirt, no water, no soap, blood, sun) it’s easy for any virus to mutate and spares to humans.
The documentary says:
“This is a wet market in the Lianghua, China. Unlike markets in much of the West, where animals are already dead when they arrive, this wet market sells meat that’s very fresh. It’s killed on sight. That’s what makes it a disease X factory. Many different animal species are stacked on top of each other, their blood and meat mixed, before being passed from human to human. All the while, their viruses are mixing and mutating, increasing the odds that one finds its way to humans.”
The wet market from Netflix’s story is in fact totally similar to the seafood market in Wuhan where coronavirus evolved.
Snakes and Bats – the Main Culprits
Scientists believe that the coronavirus (2019-nCoV) comes from snakes and bats. Both animals were sold live in the Wuhan seafood market, which made humans vulnerable to the respiratory disease.
Bats were “guilty” as well in the SARS outbreak in 2003. After several people were infected, it then transferred from humans to humans, causing a pandemic. On Thursday the newest information was that at least 170 people are dead and more than 7,000 cases have been confirmed in mainland China, as the Wuhan coronavirus spreads across Asia and the rest of the world.
The coronavirus is spreading rapidly and scientists across the globe are rushing to find a vaccine for it. The latest news says that Russia will join China’s efforts to develop a vaccine for the deadly novel coronavirus in an effort to stop spreading the disease.
A group of virologists in Australia also managed to replicate the coronavirus outside of China to help with diagnosis and help with efficient testing.
Bill Gates as Nostradamus
But, one player in Netflix’s documentary is a well-known billionaire Bill Gates who now sounds like a real live Nostradamus. He said that when a pandemic that the world has not seen before emerges, no matter the size, people regret not investing more for vaccines.
Gates said:
“If a disease comes along that we haven’t seen before, typically it would take four or five years to come up with a vaccine against that disease. And new technologies might shorten those times.”
When a pandemic comes along of any size, we always look back and wish we invested more.
The coronavirus, with its roots in Wuhan’s seafood market, eerily replicates previous virus outbreaks like the SARS virus that was also caused by live animal markets. The number of people that have been confirmed as infected by coronavirus has risen to well over 8,000, surpassing the SARS outbreak from 2002-2003 in that respect, but still with less reported deaths.
The question remains on should scientists and institutions thought before on investing more in order to prepare for potential outbreaks modeled after SARS, and would that lessened the impact of the coronavirus outbreak.
Business, News, Personal Finance
Author: Teuta Franjkovic Experienced creative professional focusing on financial and political analysis, editing daily newspapers and news sites, economical and political journalism, consulting, PR and Marketing. Teuta’s passion is to create new opportunities and bring people together.
Bill Gates Talks about Coronavirus-Like Epidemic in 2019 Netflix Documentary - Updated on Jan 31, 2020 at 8:11 am UTC by Teuta Franjkovic - In Humid Conditions the Virus EvolvesFrom eating pigeons and dogs and rats and lizards and bats – to not giving a damn about any hygiene, not to talk about any humanity when killing those animals at the spot. So yes. When Netflix describes the wet markets as a disease X factory – they couldn’t be more right. When you have such conditions (humidity, dirt, no water, no soap, blood, sun) it’s easy for any virus to mutate and spares to humans.The documentary says:“This is a wet market in the Lianghua, China. Unlike markets in much of the West, where animals are already dead when they arrive, this wet market sells meat that’s very fresh. It’s killed on sight. That’s what makes it a disease X factory. Many different animal species are stacked on top of each other, their blood and meat mixed, before being passed from human to human. All the while, their viruses are mixing and mutating, increasing the odds that one finds its way to humans.”The wet market from Netflix’s story is in fact totally similar to the seafood market in Wuhan where coronavirus evolved.Во влажных условиях вирус эволюционируетОт поедания голубей, собак, крыс, ящериц и летучих мышей-до того, чтобы не думать ни о какой гигиене, не говорить ни о какой человечности, убивая этих животных на месте. Так что да. Когда Netflix описывает влажные рынки как фабрику болезни X – они не могут быть более правы. При таких условиях (влажность, грязь, отсутствие воды, мыла, крови, солнца) любой вирус легко мутирует и щадит человека.В документальном фильме (2019) говорится::“Это мокрый рынок в Лянхуа, Китай. В отличие от рынков на большей части Запада, где животные уже мертвы, когда они прибывают, этот влажный рынок продает мясо, которое очень свежее. Его убивают с первого взгляда. Вот что делает его фабрикой болезни X. Множество различных видов животных укладываются друг на друга, их кровь и мясо смешиваются, прежде чем перейти от человека к человеку. Все это время их вирусы смешиваются и мутируют, увеличивая вероятность того, что один из них найдет свой путь к людям.”Мокрый рынок из истории Netflix на самом деле полностью похож на рынок морепродуктов в Ухане, где развился коронавирус. (November 7, 2019)
https://www.youtube.com/watch?v=OQD_-2KI244Coronavirus : la Chine en quarantaine | ARTE Reportage
ARTE
1.02M subscribers
https://www.youtube.com/watch?v=LnlRvQPP900
The Most DISGUSTING Marketing in the World - Wuhan Market (Corona Virus)
https://www.youtube.com/watch?v=G9oqvJ3iXGIConnor Reed, a British man who works at a school in Wuhan, explains how it felt to have the Covid-19 coronavirus, discusses what life is like after 40 days in lockdown and how he thinks people in the UK would cope in similar circumstances.
https://www.youtube.com/watch?v=okg7uq_HrhQHow Coronavirus Kills: Acute Respiratory Distress Syndrome (ARDS) & Treatment
29 Jan 2020
https://www.dailymail.co.uk/…/London-LOCKDOWN-Eerie-images-…
8,246 DEATHS WORLDWIDE (18 March 2020)
204,277 CASES WORLDWIDE (18 March 2020)
UK 2,626 CASES - 55 (?) DEATHS (18 March 020)
LONDON 407 CASES - 6 DEATHS
https://www.youtube.com/watch?v=VpP0Fp51Q04Coronavirus update: Wednesday, 18 March | ITV News
https://www.youtube.com/watch?v=e0OsmJTRCl8&t=127sDoctor warns of 'carnage and chaos' as UK hospitals prepare for coronavirus | ITV News
119,090 views•17 Mar 2020
https://www.youtube.com/watch?v=-e58r8x9kw8The changes the UK's supermarkets are making as demand rises amid coronavirus outbreak | ITV News
A coronavirus coup in broad daylight
As democracy goes into quarantine and surveillance of citizens becomes the norm, Israel is heading straight for an autocracy run by Benjamin Netanyahu.
By Michael Sfard March 19, 2020
")
Prime Minister Benjamin Netanyahu at a press conference about COVID-19, at the Prime Ministers Office, Jerusalem, March 11, 2020. (Flash90)https://www.972mag.com/coronavirus-netanyahu-coup-knesset/
Death by Medicine: Doctors in U.S. Responsible for a Million Deaths a Year…

Doctors Kill 1,000,000 People Each Year In the U.S. Alone – Shocking Health Statistics
TLB Editors Note: The article you are about to read was originally published in 2015, but has not received the attention it surely needs. One of our pastimes here is to go through older publications, studies and articles to find the gems like this that truly need more daylight … thus we present this in the hopes it will awaken many to the dangers of modern medicine, dangers you would never be aware of if it were not for these great doctors, researchers and authors, as well as TLB’s propensity to go looking for forgotten gems of knowledge. The vital question to be answered is … if it was known to be this bad five years ago, what the heck is it like now … ??? Please read on!Death by Medicine
By: Gary Null, PhD; Carolyn Dean MD, ND; Martin Feldman, MD; Debora Rasio, MD; and Dorothy Smith, PhD
Something is wrong when regulatory agencies pretend that vitamins are dangerous, yet ignore published statistics showing that government-sanctioned medicine is the real hazard.Until now, Life Extension could cite only isolated statistics to make its case about the dangers of conventional medicine. No one had ever analyzed and combined ALL of the published literature dealing with injuries and deaths caused by government-protected medicine. That has now changed.A group of researchers meticulously reviewed the statistical evidence and their findings are absolutely shocking.4 These researchers have authored a paper titled “Death by Medicine” that presents compelling evidence that today’s system frequently causes more harm than good.This fully referenced report shows the number of people having in-hospital, adverse reactions to prescribed drugs to be 2.2 million per year. The number of unnecessary antibiotics prescribed annually for viral infections is 20 million per year. The number of unnecessary medical and surgical procedures performed annually is 7.5 million per year. The number of people exposed to unnecessary hospitalization annually is 8.9 million per year.The most stunning statistic, however, is that the total number of deaths caused by conventional medicine is an astounding 783,936 per year. It is now evident that the American medical system is the leading cause of death and injury in the US. (By contrast, the number of deaths attributable to heart disease in 2001 was 699,697, while the number of deaths attributable to cancer was 553,251.5)We had intended to publish the entire text of “Death By Medicine” in this month’s issue. The article uncovered so many problems with conventional medicine however, that it became too long to fit within these pages. We have instead put it on our website (www.lef.org).We placed this article on our website to memorialize the failure of the American medical system. By exposing these gruesome statistics in painstaking detail, we provide a basis for competent and compassionate medical professionals to recognize the inadequacies of today’s system and at least attempt to institute meaningful reforms.Natural medicine is under siege, as pharmaceutical company lobbyists urge lawmakers to deprive Americans of the benefits of dietary supplements. Drug-company front groups have launched slanderous media campaigns to discredit the value of healthy lifestyles. The FDA continues to interfere with those who offer natural products that compete with prescription drugs.These attacks against natural medicine obscure a lethal problem that until now was buried in thousands of pages of scientific text. In response to these baseless challenges to natural medicine, the Nutrition Institute of America commissioned an independent review of the quality of “government-approved” medicine. The startling findings from this meticulous study indicate that conventional medicine is “the leading cause of death” in the United States .The Nutrition Institute of America is a nonprofit organization that has sponsored independent research for the past 30 years. To support its bold claim that conventional medicine is America ‘s number-one killer, the Nutritional Institute of America mandated that every “count” in this “indictment” of US medicine be validated by published, peer-reviewed scientific studies.What you are about to read is a stunning compilation of facts that documents that those who seek to abolish consumer access to natural therapies are misleading the public. Over 700,000 Americans die each year at the hands of government-sanctioned medicine, while the FDA and other government agencies pretend to protect the public by harassing those who offer safe alternatives.A definitive review of medical peer-reviewed journals and government health statistics shows that American medicine frequently causes more harm than good.Each year approximately 2.2 million US hospital patients experience adverse drug reactions (ADRs) to prescribed medications.(1) In 1995, Dr. Richard Besser of the federal Centers for Disease Control and Prevention (CDC) estimated the number of unnecessary antibiotics prescribed annually for viral infections to be 20 million; in 2003, Dr. Besser spoke in terms of tens of millions of unnecessary antibiotics prescribed annually.(2, 2a) Approximately 7.5 million unnecessary medical and surgical procedures are performed annually in the US,(3) while approximately 8.9 million Americans are hospitalized unnecessarily.(4)Iatrogenic: “Induced by a physician’s words or therapy (used especially of a complication resulting from treatment)”As shown in the following table, the estimated total number of iatrogenic deaths—that is, deaths induced inadvertently by a physician or surgeon or by medical treatment or diagnostic procedures— in the US annually is 783,936. It is evident that the American medical system is itself the leading cause of death and injury in the US . By comparison, approximately 699,697 Americans died of heart in 2001, while 553,251 died of cancer.(5)Table 1: Estimated Annual Mortality and Economic Cost of Medical InterventionCondition Deaths Cost Author Adverse Drug Reactions 106,000 $12 billion Lazarou (1), Suh (49) Medical Error 98,000 $2 billion IOM(6) Bedsores 115,000 $55 billion Zakellis(7), Barczak(8) Infection 88,000 $5 billion Weinstein(9), MMWR(10) Malnutrition 108,800 – Nurses Coalition(11) Outpatients 199,000 $77 billion Starfield(12), Weingart(112) Unnecessary Procedures 37,136 $122 billion HCUP(3,13) Surgery-Related 32,000 $9 billion AHRQ(85) Total 783,936 $282 billion  Using Leape’s 1997 medical and drug error rate of 3 million(14) multiplied by the 14% fatality rate he used in 1994(16) produces an annual death rate of 420,000 for drug errors and medical errors combined. Using this number instead of Lazorou’s 106,000 drug errors and the Institute of Medicine ‘s (IOM) estimated 98,000 annual medical errors would add another 216,000 deaths, for a total of 999,936 deaths annually.Table 2: Estimated Annual Mortality and Economic Cost of Medical Intervention
Using Leape’s 1997 medical and drug error rate of 3 million(14) multiplied by the 14% fatality rate he used in 1994(16) produces an annual death rate of 420,000 for drug errors and medical errors combined. Using this number instead of Lazorou’s 106,000 drug errors and the Institute of Medicine ‘s (IOM) estimated 98,000 annual medical errors would add another 216,000 deaths, for a total of 999,936 deaths annually.Table 2: Estimated Annual Mortality and Economic Cost of Medical InterventionCondition Deaths Cost Author ADR/Medical error 420,000 $200 billion Leap(14) Bedsores 115,000 $55 billion Zakesslis(7), Barczak(8) Infection 88,000 $5 billion Weinstein(9), MMWR(1o) Malnutrition 108,800 — Nurses Coalition(11) Outpatients 199,000 $77 billion Starfield(12), Weingart(112) Unnecessary Procedures 37,136 $122 billion HCUP(3,13) Surgery-Related 32,000 $9 billion AHRQ(85) Total 999,936 $468 billion (Webmaster’s Note: I rounded off the above figure of 999,936 to 1,000,000 for the title of this article).The enumerating of unnecessary medical events is very important in our analysis. Any invasive, unnecessary medical procedure must be considered as part of the larger iatrogenic picture. Unfortunately, cause and effect go unmonitored. The figures on unnecessary events represent people who are thrust into a dangerous health care system. Each of these 16.4 million lives is being affected in ways that could have fatal consequences. Simply entering a hospital could result in the following:- In 16.4 million people, a 2.1% chance (affecting 186,000) of a serious adverse drug reaction(1)
- In 16.4 million people, a 5-6% chance (affecting 489,500) of acquiring a nosocomial* infection(9)
- In 16.4 million people, a 4-36% chance (affecting 1.78 million) of having an iatrogenic injury (medical error and adverse drug reactions).(16)
- In 16.4 million people, a 17% chance (affecting 1.3 million) of a procedure error.(40)
Noscocomial: Taking place or originating in a hospital.These statistics represent a one-year time span. Working with the most conservative figures from our statistics, we project the following 10-year death rates.Table 3: Estimated 10-Year Death Rates from Medical InterventionCondition 10-Year Deaths Author Adverse Drug Reaction 1.06 million (1) Medical error 0.98 million (6) Bedsores 1.15 million (7,8) Nosocomial Infection 0.88 million (9,10) Malnutrition 1.09 million (11) Outpatients 1.99 million (12,112) Unnecessary Procedures 371,360 (3,13) Surgery-related 320,000 (85) Total 7,841,360 Our estimated 10-year total of 7.8 million iatrogenic deaths is more than all the casualties from all the wars fought by the US throughout its entire history.Our projected figures for unnecessary medical events occurring over a 10-year period also are dramatic.Table 4: Estimated 10-Year Unnecessary Medical EventsUnnecessary Events 10-year Number Iatrogenic Events Hospitalization 89 million (4) 17 million Procedures 75 million (3) 15 million Total 163 million These figures show that an estimated 164 million people—more than half of the total US population—receive unneeded medical treatment over the course of a decade.INTRODUCTIONNever before have the complete statistics on the multiple causes of iatrogenesis been combined in one article. Medical science amasses tens of thousands of papers annually, each representing a tiny fragment of the whole picture. To look at only one piece and try to understand the benefits and risks is like standing an inch away from an elephant and trying to describe everything about it. You have to step back to see the big picture, as we have done here. Each specialty, each division of medicine keeps its own records and data on morbidity and mortality. We have now completed the painstaking work of reviewing thousands of studies and putting pieces of the puzzle together.IS AMERICAN MEDICINE WORKING?US health care spending reached $1.6 trillion in 2003, representing 14% of the nation’s gross national product.(15) Considering this enormous expenditure, we should have the best medicine in the world. We should be preventing and reversing disease, and doing minimal harm. Careful and objective review, however, shows we are doing the opposite. Because of the extraordinarily narrow, technologically driven context in which contemporary medicine examines the human condition, we are completely missing the larger picture.Medicine is not taking into consideration the following critically important aspects of a healthy human organism: (a) stress and how it adversely affects the immune system and life processes; (b) insufficient exercise; (c) excessive caloric intake; (d) highly processed and denatured foods grown in denatured and chemically damaged soil; and (e) exposure to tens of thousands of environmental toxins. Instead of minimizing these disease-causing factors, we cause more illness through medical technology, diagnostic testing, overuse of medical and surgical procedures, and overuse of pharmaceutical drugs. The huge disservice of this therapeutic strategy is the result of little effort or money being spent on preventing disease.UNDERREPORTING OF IATROGENIC EVENTSAs few as 5% and no more than 20% of iatrogenic acts are ever reported.(16,24,25,33,34)This implies that if medical errors were completely and accurately reported, we would have an annual iatrogenic death toll much higher than 783,936. In 1994, Leape said his figure of 180,000 medical mistakes resulting in death annually was equivalent to three jumbo-jet crashes every two days.(16) Our considerably higher figure is equivalent to six jumbo jets are falling out of the sky each day.What we must deduce from this report is that medicine is in need of complete and total reform—from the curriculum in medical schools to protecting patients from excessive medical intervention. It is obvious that we cannot change anything if we are not honest about what needs to be changed. This report simply shows the degree to which change is required.We are fully aware of what stands in the way of change: powerful pharmaceutical and medical technology companies, along with other powerful groups with enormous vested interests in the business of medicine. They fund medical research, support medical schools and hospitals, and advertise in medical journals. With deep pockets, they entice scientists and academics to support their efforts. Such funding can sway the balance of opinion from professional caution to uncritical acceptance of new therapies and drugs. You have only to look at the people who make up the hospital, medical, and government health advisory boards to see conflicts of interest. The public is mostly unaware of these interlocking interests.For example, a 2003 study found that nearly half of medical school faculty who serve on institutional review boards (IRB) to advise on clinical trial research also serve as consultants to the pharmaceutical industry.(17) The study authors were concerned that such representation could cause potential conflicts of interest. A news release by Dr. Erik Campbell, the lead author, said, “Our previous research with faculty has shown us that ties to industry can affect scientific behavior, leading to such things as trade secrecy and delays in publishing research. It’s possible that similar relationships with companies could affect IRB members’ activities and attitudes.”(18)MEDICAL ETHICS AND CONFLICT OF INTEREST IN SCIENTIFIC MEDICINEJonathan Quick, director of essential drugs and medicines policy for the World Health Organization (WHO), wrote in a recent WHO bulletin: “If clinical trials become a commercial venture in which self-interest overrules public interest and desire overrules science, then the social contract which allows research on human subjects in return for medical advances is broken.”(19)As former editor of the New England Journal of Medicine, Dr. Marcia Angell struggled to bring greater attention to the problem of commercializing scientific research. In her outgoing editorial entitled “Is Academic Medicine for Sale?”Angell said that growing conflicts of interest are tainting science and called for stronger restrictions on pharmaceutical stock ownership and other financial incentives for researchers:(20) “When the boundaries between industry and academic medicine become as blurred as they are now, the business goals of industry influence the mission of medical schools in multiple ways.” She did not discount the benefits of research but said a Faustian bargain now existed between medical schools and the pharmaceutical industry.Angell left the New England Journal in June 2000. In June 2002, the New England Journal of Medicine announced that it would accept journalists who accept money from drug companies because it was too difficult to find ones who have no ties. Another former editor of the journal, Dr. Jerome Kassirer, said that was not the case and that plenty of researchers are available who do not work for drug companies.(21) According to an ABC news report, pharmaceutical companies spend over $2 billion a year on over 314,000 events attended by doctors.The ABC news report also noted that a survey of clinical trials revealed that when a drug company funds a study, there is a 90% chance that the drug will be perceived as effective whereas a non-drug-company-funded study will show favorable results only 50% of the time. It appears that money can’t buy you love but it can buy any “scientific” result desired.Cynthia Crossen, a staffer for the Wall Street Journal, in 1996 published Tainted Truth : The Manipulation of Fact in America , a book about the widespread practice of lying with statistics.(22) Commenting on the state of scientific research, she wrote: “The road to hell was paved with the flood of corporate research dollars that eagerly filled gaps left by slashed government research funding.” Her data on financial involvement showed that in l981 the drug industry “gave” $292 million to colleges and universities for research. By l991, this figure had risen to $2.1 billion.THE FIRST IATROGENIC STUDYDr. Lucian L. Leape opened medicine’s Pandora’s box in his 1994 paper, “Error in Medicine,” which appeared in the Journal of the American Medical Association (JAMA).(16) He found that Schimmel reported in 1964 that 20% of hospital patients suffered iatrogenic injury, with a 20% fatality rate. In 1981 Steel reported that 36% of hospitalized patients experienced iatrogenesis with a 25% fatality rate, and adverse drug reactions were involved in 50% of the injuries. In 1991, Bedell reported that 64% of acute heart attacks in one hospital were preventable and were mostly due to adverse drug reactions.Leape focused on the “Harvard Medical Practice Study” published in 1991, (16a) which found a 4% iatrogenic injury rate for patients, with a 14% fatality rate, in 1984 in New York State. From the 98,609 patients injured and the 14% fatality rate, he estimated that in the entire U.S. 180,000 people die each year partly as a result of iatrogenic injury.Why Leape chose to use the much lower figure of 4% injury for his analysis remains in question. Using instead the average of the rates found in the three studies he cites (36%, 20%, and 4%) would have produced a 20% medical error rate. The number of iatrogenic deaths using an average rate of injury and his 14% fatality rate would be 1,189,576.Leape acknowledged that the literature on medical errors is sparse and represents only the tip of the iceberg, noting that when errors are specifically sought out, reported rates are “distressingly high.” He cited several autopsy studies with rates as high as 35-40% of missed diagnoses causing death. He also noted that an intensive care unit reported an average of 1.7 errors per day per patient, and 29% of those errors were potentially serious or fatal.Leape calculated the error rate in the intensive care unit study. First, he found that each patient had an average of 178 “activities” (staff/procedure/medical interactions) a day, of which 1.7 were errors, which means a 1% failure rate. This may not seem like much, but Leape cited industry standards showing that in aviation, a 0.1% failure rate would mean two unsafe plane landings per day at Chicago’s O’Hare International Airport; in the US Postal Service, a 0.1% failure rate would mean 16,000 pieces of lost mail every hour; and in the banking industry, a 0.1% failure rate would mean 32,000 bank checks deducted from the wrong bank account.In trying to determine why there are so many medical errors, Leape acknowledged the lack of reporting of medical errors. Medical errors occur in thousands of different locations and are perceived as isolated and unusual events. But the most important reason that the problem of medical errors is unrecognized and growing, according to Leape, is that doctors and nurses are unequipped to deal with human error because of the culture of medical training and practice.Doctors are taught that mistakes are unacceptable. Medical mistakes are therefore viewed as a failure of character and any error equals negligence. No one is taught what to do when medical errors do occur. Leape cites McIntyre and Popper, who said the “infallibility model” of medicine leads to intellectual dishonesty with a need to cover up mistakes rather than admit them. There are no Grand Rounds on medical errors, no sharing of failures among doctors, and no one to support them emotionally when their error harms a patient.Leape hoped his paper would encourage medical practitioners “to fundamentally change the way they think about errors and why they occur.” It has been almost a decade since this groundbreaking work, but the mistakes continue to soar.In 1995, a JAMA report noted, “Over a million patients are injured in US hospitals each year, and approximately 280,000 die annually as a result of these injuries. Therefore, the iatrogenic death rate dwarfs the annual automobile accident mortality rate of 45,000 and accounts for more deaths than all other accidents combined.”(23)At a 1997 press conference, Leape released a nationwide poll on patient iatrogenesis conducted by the National Patient Safety Foundation (NPSF), which is sponsored by the American Medical Association (AMA). Leape is a founding member of NPSF. The survey found that more than 100 million Americans have been affected directly or indirectly by a medical mistake. Forty-two percent were affected directly and 84% personally knew of someone who had experienced a medical mistake.(14)At this press conference, Leape updated his 1994 statistics, noting that as of 1997, medical errors in inpatient hospital settings nationwide could be as high as 3 million and could cost as much as $200 billion . Leape used a 14% fatality rate to determine a medical error death rate of 180,000 in 1994.(16) In 1997, using Leape’s base number of 3 million errors, the annual death rate could be as high as 420,000 for hospital inpatients alone.ONLY A FRACTION OF MEDICAL ERRORS ARE REPORTEDIn 1994, Leape said he was well aware that medical errors were not being reported.(16) A study conducted in two obstetrical units in the UK found that only about one-quarter of adverse incidents were ever reported, to protect staff, preserve reputations, or for fear of reprisals, including lawsuits.(24). An analysis by Wald and Shojania found that only 1.5% of all adverse events result in an incident report, and only 6% of adverse drug events are identified properly.The authors learned that the American College of Surgeons estimates that surgical incident reports routinely capture only 5-30% of adverse events. In one study, only 20% of surgical complications resulted in discussion at morbidity and mortality rounds.(25) From these studies, it appears that all the statistics gathered on medical errors may substantially underestimate the number of adverse drug and medical therapy incidents. They also suggest that our statistics concerning mortality resulting from medical errors may be in fact be conservative figures.An article in Psychiatric Times (April 2000) outlines the stakes involved in reporting medical errors.(26) The authors found that the public is fearful of suffering a fatal medical error, and doctors are afraid they will be sued if they report an error. This brings up the obvious question: who is reporting medical errors? Usually it is the patient or the patient’s surviving family. If no one notices the error, it is never reported.Janet Heinrich, an associate director at the U.S. General Accounting Office responsible for health financing and public health issues, testified before a House subcommittee hearing on medical errors that “the full magnitude of their threat to the American public is unknown” and “gathering valid and useful information about adverse events is extremely difficult.” She acknowledged that the fear of being blamed, and the potential for legal liability, played key roles in the underreporting of errors. The Psychiatric Times noted that the AMA strongly opposes mandatory reporting of medical errors.(26) If doctors are not reporting, what about nurses? A survey of nurses found that they also fail to report medical mistakes for fear of retaliation.(27)Standard medical pharmacology texts admit that relatively few doctors ever report adverse drug reactions to the FDA.(28) The reasons range from not knowing such a reporting system exists to fear of being sued.(29) Yet the public depends on this tremendously flawed system of voluntary reporting by doctors to know whether a drug or a medical intervention is harmful.Pharmacology texts also will tell doctors how hard it is to separate drug side effects from disease symptoms. Treatment failure is most often attributed to the disease and not the drug or doctor. Doctors are warned, “Probably nowhere else in professional life are mistakes so easily hidden, even from ourselves.”(30) It may be hard to accept, but it is not difficult to understand why only 1 in 20 side effects is reported to either hospital administrators or the FDA.(31, 31a)If hospitals admitted to the actual number of errors for which they are responsible, which is about 20 times what is reported, they would come under intense scrutiny.(32) Jerry Phillips, associate director of the FDA’s Office of Post Marketing Drug Risk Assessment, confirms this number. “In the broader area of adverse drug reaction data, the 250,000 reports received annually probably represent only 5% of the actual reactions that occur.”(33) Dr. Jay Cohen, who has extensively researched adverse drug reactions, notes that because only 5% of adverse drug reactions are reported, there are in fact 5 million medication reactions each year.(34)A 2003 survey is all the more distressing because there seems to be no improvement in error reporting, even with all the attention given to this topic. Dr. Dorothea Wild surveyed medical residents at a community hospital in Connecticut and found that only half were aware that the hospital had a medical error-reporting system, and that the vast majority did not use it at all. Dr. Wild says this does not bode well for the future. If doctors don’t learn error reporting in their training, they will never use it. Wild adds that error reporting is the first step in locating the gaps in the medical system and fixing them. Not even that first step has been taken to date.(35)PUBLIC SUGGESTIONS ON IATROGENESISIn a telephone survey, 1,207 adults ranked the effectiveness of the following measures in reducing preventable medical errors that result in serious harm.(36) (Following each measure is the percentage of respondents who ranked the measure as “very effective.”)- Giving doctors more time to spend with patients (78%)
- Requiring hospitals to develop systems to avoid medical errors (74%)
- better training of health professionals (73%)
- Using only doctors specially trained in intensive care medicine on intensive care units (73%)
- Requiring hospitals to report all serious medical errors to a state agency (71%)
- Increasing the number of hospital nurses (69%)
- Reducing the work hours of doctors in training to avoid fatigue (66%)
- encouraging hospitals to voluntarily report serious medical errors to a state agency (62%).
DRUG IATROGENESISPrescription drugs constitute the major treatment modality of scientific medicine. With the discovery of the “germ theory,” medical scientists convinced the public that infectious organisms were the cause of illness. Finding the “cure” for these infections proved much harder than anyone imagined. From the beginning, chemical drugs promised much more than they delivered. But far beyond not working, the drugs also caused incalculable side effects. The drugs themselves, even when properly prescribed, have side effects that can be fatal, as Lazarou’s study(1) showed. But human error can make the situation even worse.MEDICATION ERRORSA survey of a 1992 national pharmacy database found a total of 429,827 medication errors from 1,081 hospitals. Medication errors occurred in 5.22% of patients admitted to these hospitals each year. The authors concluded that at least 90,895 patients annually were harmed by medication errors in the US as a whole.(37)A 2002 study shows that 20% of hospital medications for patients had dosage errors. Nearly 40% of these errors were considered potentially harmful to the patient. In a typical 300-patient hospital, the number of errors per day was 40.(38)Problems involving patients’ medications were even higher the following year. The error rate intercepted by pharmacists in this study was 24%, making the potential minimum number of patients harmed by prescription drugs 417,908.(39)RECENT ADVERSE DRUG REACTIONSMore-recent studies on adverse drug reactions show that the figures from 1994 published in Lazarou’s 1998 JAMA article may be increasing. A 2003 study followed 400 patients after discharge from a tertiary care hospital setting (requiring highly specialized skills, technology, or support services). Seventy-six patients (19%) had adverse events. Adverse drug events were the most common, at 66% of all events. The next most common event was procedure-related injuries, at 17%.(40)In a New England Journal of Medicine study, an alarming one in four patients suffered observable side effects from the more than 3.34 billion prescription drugs filled in 2002.(41) One of the doctors who produced the study was interviewed by Reuters and commented, “With these 10-minute appointments, it’s hard for the doctor to get into whether the symptoms are bothering the patients.”(42) William Tierney, who editorialized on the New England Journal study, said “… given the increasing number of powerful drugs available to care for the aging population, the problem will only get worse.”The drugs with the worst record of side effects were selective serotonin reuptake inhibitors ( SSRIs), nonsteroidal anti-inflammatory drugs (NSAIDs), and calcium-channel blockers. Reuters also reported that prior research has suggested that nearly 5% of hospital admissions (over 1 million per year) are the result of drug side effects. But most of the cases are not documented as such. The study found that one of the reasons for this failure is that in nearly two-thirds of the cases, doctors could not diagnose drug side effects or the side effects persisted because the doctor failed to heed the warning signs.MEDICATING OUR FEELINGSPatients seeking a more joyful existence and relief from worry, stress, and anxiety often fall victim to the messages endlessly displayed on TV and billboards. Often, instead of gaining relief, they fall victim to the myriad iatrogenic side effects of antidepressant medication.Moreover, a whole generation of antidepressant users has been created from young people growing up on Ritalin. Medicating youth and modifying their emotions must have some impact on how they learn to deal with their feelings. They learn to equate coping with drugs rather than with their inner resources. As adults, these medicated youth reach for alcohol, drugs, or even street drugs to cope. According to JAMA , “Ritalin acts much like cocaine.”(43) Today’s marketing of mood-modifying drugs such as Prozac and Zoloft ® makes them not only socially acceptable but almost a necessity in today’s stressful world.TELEVISION DIAGNOSISTo reach the widest audience possible, drug companies are no longer just targeting medical doctors with their marketing of antidepressants. By 1995, drug companies had tripled the amount of money allotted to direct advertising of prescription drugs to consumers. The majority of this money is spent on seductive television ads. From 1996 to 2000, spending rose from $791 million to nearly $2.5 billion.(44) This $2.5 billion represents only 15% of the total pharmaceutical advertising budget.While the drug companies maintain that direct-to-consumer advertising is educational, Dr. Sidney M. Wolfe of the Public Citizen Health Research Group in Washington, DC, argues that the public often is misinformed about these ads.(45) People want what they see on television and are told to go to their doctors for a prescription. Doctors in private practice either acquiesce to their patients’ demands for these drugs or spend valuable time trying to talk patients out of unnecessary drugs.Dr. Wolfe remarks that one important study found that people mistakenly believe that the “FDA reviews all ads before they are released and allows only the safest and most effective drugs to be promoted directly to the public.”(46)HOW DO WE KNOW DRUGS ARE SAFE?Another aspect of scientific medicine that the public takes for granted is the testing of new drugs. Drugs generally are tested on individuals who are fairly healthy and not on other medications that could interfere with findings. But when these new drugs are declared “safe” and enter the drug prescription books, they are naturally going to be used by people who are on a variety of other medications and have a lot of other health problems. Then a new phase of drug testing called “post-approval” comes into play, which is the documentation of side effects once drugs hit the market.In one very telling report, the federal government’s General Accounting Office “found that of the 198 drugs approved by the FDA between 1976 and 1985… 102 (or 51.5%) had serious post-approval risks… the serious post-approval risks (included) heart failure, myocardial infarction, anaphylaxis, respiratory depression and arrest, seizures, kidney and liver failure, severe blood disorders, birth defects and fetal toxicity, and blindness.”(47)NBC Television’s investigative show “Dateline” wondered if your doctor is moonlighting as a drug company representative. After a yearlong investigation, NBC reported that because doctors can legally prescribe any drug to any patient for any condition, drug companies heavily promote “off label” and frequently inappropriate and untested uses of these medications, even though these drugs are approved only for the specific indications for which they have been tested.(48)The leading causes of adverse drug reactions are antibiotics (17%), cardiovascular drugs (17%), chemotherapy (15%), and analgesics and anti-inflammatory agents (15%).(49)SPECIFIC DRUG IATROGENESIS: ANTIBIOTICSAccording to William Agger, MD, director of microbiology and chief of infectious disease at Gundersen Lutheran Medical Center in La Crosse, WI, 30 million pounds of antibiotics are used in America each year.(50) Of this amount, 25 million pounds are used in animal husbandry, and 23 million pounds are used to try to prevent disease and the stress of shipping, as well as to promote growth. Only 2 million pounds are given for specific animal infections. Dr. Agger reminds us that low concentrations of antibiotics are measurable in many of our foods and in various waterways around the world, much of it seeping in from animal farms.Agger contends that overuse of antibiotics results in food-borne infections resistant to antibiotics. Salmonella is found in 20% of ground meat, but the constant exposure of cattle to antibiotics has made 84% of salmonella resistant to at least one anti-salmonella antibiotic. Diseased animal food accounts for 80% of salmonellosis in humans, or 1.4 million cases per year. The conventional approach to countering this epidemic is to radiate food to try to kill all organisms while continuing to use the antibiotics that created the problem in the first place. Approximately 20% of chickens are contaminated with Campylobacter jejuni, an organism that causes 2.4 million cases of illness annually. Fifty-four percent of these organisms are resistant to at least one anti-campylobacter antimicrobial agent.Denmark banned growth-promoting antibiotics beginning in 1999, which cut their use by more than half within a year, from 453,200 to 195,800 pounds. A report from Scandinavia found that removing antibiotic growth promoters had no or minimal effect on food production costs. Agger warns that the current crowded, unsanitary methods of animal farming in the US support constant stress and infection, and are geared toward high antibiotic use.In the US, over 3 million pounds of antibiotics are used every year on humans. With a population of 284 million Americans, this amount is enough to give every man, woman, and child 10 teaspoons of pure antibiotics per year. Agger says that exposure to a steady stream of antibiotics has altered pathogens such as Streptococcus pneumoniae, Staplococcus aureus, and entercocci, to name a few.Almost half of patients with upper respiratory tract infections in the U.S. still receive antibiotics from their doctor.(51) According to the CDC, 90% of upper respiratory infections are viral and should not be treated with antibiotics. In Germany, the prevalence of systemic antibiotic use in children aged 0-6 years was 42.9%.(52)Data obtained from nine US health insurers on antibiotic use in 25,000 children from 1996 to 2000 found that rates of antibiotic use decreased. Antibiotic use in children aged three months to under 3 years decreased 24%, from 2.46 to 1.89 antibiotic prescriptions per patient per year. For children aged 3 to under 6 years, there was a 25% reduction from 1.47 to 1.09 antibiotic prescriptions per patient per year. And for children aged 6 to under 18 years, there was a 16% reduction from 0.85 to 0.69 antibiotic prescriptions per patient per year.(53) Despite these reductions, the data indicate that on average every child in America receives 1.22 antibiotic prescriptions annually.Group A beta-hemolytic streptococci is the only common cause of sore throat that requires antibiotics, with penicillin and erythromycin the only recommended treatment. Ninety percent of sore-throat cases, however, are viral. Antibiotics were used in 73% of the estimated 6.7 million adult annual visits for sore throat in the US between 1989 and 1999. Furthermore, patients treated with antibiotics were prescribed non-recommended broad-spectrum antibiotics in 68% of visits. This period saw a significant increase in the use of newer, more expensive broad-spectrum antibiotics and a decrease in use of the recommended antibiotics penicillin and erythromycin.(54) A ntibiotics being prescribed in 73% of sore-throat cases instead of the recommended 10% resulted in a total of 4.2 million unnecessary antibiotic prescriptions from 1989 to 1999.THE PROBLEM WITH ANTIBIOTICSIn September 2003, the CDC re-launched a program started in 1995 called “Get Smart: Know When Antibiotics Work.”(55) This $1.6 million campaign is designed to educate patients about the overuse and inappropriate use of antibiotics. Most people involved with alternative medicine have known about the dangers of antibiotic overuse for decades. Finally the government is focusing on the problem, yet it is spending only a miniscule amount of money on an iatrogenic epidemic that is costing billions of dollars and thousands of lives.The CDC warns that 90% of upper respiratory infections, including children’s ear infections, are viral and that antibiotics do not treat viral infection. More than 40% of about 50 million prescriptions for antibiotics written each year in physicians’ offices are inappropriate.(2) Using antibiotics when not needed can lead to the development of deadly strains of bacteria that are resistant to drugs and cause more than 88,000 deaths due to hospital-acquired infections.(9) The CDC, however, seems to be blaming patients for misusing antibiotics even though they are available only by prescription from physicians.According to Dr. Richard Besser, head of “Get Smart”: “Programs that have just targeted physicians have not worked. Direct-to-consumer advertising of drugs is to blame in some cases.” Besser says the program “teaches patients and the general public that antibiotics are precious resources that must be used correctly if we want to have them around when we need them. Hopefully, as a result of this campaign, patients will feel more comfortable asking their doctors for the best care for their illnesses, rather than asking for antibiotics.”(56)What constitutes the “best care”? The CDC does not elaborate and ignores the latest research on the dozens of nutraceuticals that have been scientifically proven to treat viral infections and boost immune-system function. Will doctors recommend vitamin C, echinacea, elderberry, vitamin A, zinc, or homeopathic oscillococcinum? Probably not. The CDC’s common-sense recommendations that most people follow anyway include getting proper rest, drinking plenty of fluids, and using a humidifier.The pharmaceutical industry claims it supports limiting the use of antibiotics. The drug company Bayer sponsors a program called “Operation Clean Hands” through an organization called LIBRA.(57) The CDC also is involved in trying to minimize antibiotic resistance, but nowhere in its publications is there any reference to the role of nutraceuticals in boosting the immune system, nor to the thousands of journal articles that support this approach. This tunnel vision and refusal to recommend the available non-drug alternatives is unfortunate when the CDC is desperately trying to curb the overuse of antibiotics.DRUGS POLLUTE OUR WATER SUPPLYWe have reached the point of saturation with prescription drugs. Every body of water tested contains measurable drug residues. The tons of antibiotics used in animal farming, which run off into the water table and surrounding bodies of water, are conferring antibiotic resistance to germs in sewage, and these germs also are found in our water supply. Flushed down our toilets are tons of drugs and drug metabolites that also find their way into our water supply. We have no way to know the long-term health consequences of ingesting a mixture of drugs and drug-breakdown products. These drugs represent another level of iatrogenic disease that we are unable to completely measure.(58-67)SPECIFIC DRUG IATROGENESIS: NSAIDsIt’s not just the US that is plagued by iatrogenesis. A survey of more than 1,000 French general practitioners (GPs) tested their basic pharmacological knowledge and practice in prescribing NSAIDs, which rank first among commonly prescribed drugs for serious adverse reactions. The study results suggest that GPs do not have adequate knowledge of these drugs and are unable to effectively manage adverse reactions.(68)A cross-sectional survey of 125 patients attending specialty pain clinics in South London found that possible iatrogenic factors such as “over-investigation, inappropriate information, and advice given to patients as well as misdiagnosis, over-treatment, and inappropriate prescription of medication were common.”(69)SPECIFIC DRUG IATROGENESIS: CANCER CHEMOTHERAPYIn 1989, German biostatistician Ulrich Abel, PhD, wrote a monograph entitled “Chemotherapy of Advanced Epithelial Cancer.” It was later published in shorter form in a peer-reviewed medical journal.(70) Abel presented a comprehensive analysis of clinical trials and publications representing over 3,000 articles examining the value of cytotoxic chemotherapy on advanced epithelial cancer. Epithelial cancer is the type of cancer with which we are most familiar, arising from epithelium found in the lining of body organs such as the breast, prostate, lung, stomach, and bowel. From these sites, cancer usually infiltrates adjacent tissue and spreads to the bone, liver, lung, or brain.With his exhaustive review, Abel concluded there is no direct evidence that chemotherapy prolongs survival in patients with advanced carcinoma; in small-cell lung cancer and perhaps ovarian cancer, the therapeutic benefit is only slight. According to Abel, “Many oncologists take it for granted that response to therapy prolongs survival, an opinion which is based on a fallacy and which is not supported by clinical studies.”Over a decade after Abel’s exhaustive review of chemotherapy, there seems no decrease in its use for advanced carcinoma. For example, when conventional chemotherapy and radiation have not worked to prevent metastases in breast cancer, high-dose chemotherapy (HDC) along with stem-cell transplant (SCT) is the treatment of choice. In March 2000, however, results from the largest multi-center randomized controlled trial conducted thus far showed that, compared to a prolonged course of monthly conventional-dose chemotherapy, HDC and SCT were of no benefit, (71) with even a slightly lower survival rate for the HDC/SCT group. Serious adverse effects occurred more often in the HDC group than the standard-dose group. One treatment-related death (within 100 days of therapy) was recorded in the HDC group, but none was recorded in the conventional chemotherapy group. The women in this trial were highly selected as having the best chance to respond.Unfortunately, no all-encompassing follow-up study such as Dr. Abel’s exists to indicate whether there has been any improvement in cancer-survival statistics since 1989. In fact, research should be conducted to determine whether chemotherapy itself is responsible for secondary cancers instead of progression of the original disease. We continue to question why well-researched alternative cancer treatments are not used.DRUG COMPANIES FINEDPeriodically, the FDA fines a drug manufacturer when its abuses are too glaring and impossible to cover up. In May 2002, The Washington Post reported that Schering-Plough Corp., the maker of Claritin, was to pay a $500 million dollar fine to the FDA for quality-control problems at four of its factories.(72) The indictment came after the Public Citizen Health Research Group, led by Dr. Sidney Wolfe, called for a criminal investigation of Schering-Plough, charging that the company distributed albuterol asthma inhalers even though it knew the units were missing the active ingredient.The FDA tabulated infractions involving 125 products, or 90% of the drugs made by Schering-Plough since 1998. Besides paying the fine, the company was forced to halt the manufacture of 73 drugs or suffer another $175 million fine. Schering-Plough’s news releases told another story, assuring consumers that they should still feel confident in the company’s products.This large settlement served as a warning to the drug industry about maintaining strict manufacturing practices and has given the FDA more clout in dealing with drug company compliance. According to The Washington Post article, a federal appeals court ruled in 1999 that the FDA could seize the profits of companies that violate “good manufacturing practices.” Since that time, Abbott Laboratories has paid a $100 million fine for failing to meet quality standards in the production of medical test kits, while Wyeth Laboratories paid $30 million in 2000 to settle accusations of poor manufacturing practices.UNNECESSARY SURGICAL PROCEDURESIn 1974, 2.4 million unnecessary surgeries were performed, resulting in 11,900 deaths at a cost of $3.9 billion.(73,74) In 2001, 7.5 million unnecessary surgical procedures were performed, resulting in 37,136 deaths at a cost of $122 billion (using 1974 dollars).(3)It is very difficult to obtain accurate statistics when studying unnecessary surgery. In 1989, Leape wrote that perhaps 30% of controversial surgeries—which include cesarean section, tonsillectomy, appendectomy, hysterectomy, gastrectomy for obesity, breast implants, and elective breast implants(74)— are unnecessary. In 1974, the Congressional Committee on Interstate and Foreign Commerce held hearings on unnecessary surgery. It found that 17.6% of recommendations for surgery were not confirmed by a second opinion. The House Subcommittee on Oversight and Investigations extrapolated these figures and estimated that, on a nationwide basis, there were 2.4 million unnecessary surgeries performed annually, resulting in 11,900 deaths at an annual cost of $3.9 billion.(73)According to the Healthcare Cost and Utilization Project within the Agency for Healthcare Research and Quality(13), in 2001 the 50 most common medical and surgical procedures were performed approximately 41.8 million times in the US. Using the 1974 House Subcommittee on Oversight and Investigations’ figure of 17.6% as the percentage of unnecessary surgical procedures, and extrapolating from the death rate in 1974, produces nearly 7.5 million (7,489,718) unnecessary procedures and a death rate of 37,136, at a cost of $122 billion (using 1974 dollars).In 1995, researchers conducted a similar analysis of back surgery procedures, using the 1974 “unnecessary surgery percentage” of 17.6. Testifying before the Department of Veterans Affairs, they estimated that of the 250,000 back surgeries performed annually in the US at a hospital cost of $11,000 per patient, the total number of unnecessary back surgeries approaches 44,000, costing as much as $484 million.(75)Like prescription drug use driven by television advertising, unnecessary surgeries are escalating. Media-driven surgery such as gastric bypass for obesity “modeled” by Hollywood celebrities seduces obese people to think this route is safe and sexy. Unnecessary surgeries have even been marketed on the Internet.(76) A study in Spain declares that 20-25% of total surgical practice represents unnecessary operations.(77)According to data from the National Center for Health Statistics for 1979 to 1984, the total number of surgical procedures increased 9% while the number of surgeons grew 20%. The study notes that the large increase in the number of surgeons was not accompanied by a parallel increase in the number of surgeries performed, and expressed concern about an excess of surgeons to handle the surgical caseload.(78)From 1983 to 1994, however, the incidence of the 10 most commonly performed surgical procedures jumped 38%, to 7,929,000 from 5,731,000 cases. By 1994, cataract surgery was the most common procedure with more than 2 million operations, followed by cesarean section (858,000 procedures) and inguinal hernia operations (689,000 procedures). Knee arthroscopy procedures increased 153% while prostate surgery declined 29%.(79)The list of iatrogenic complications from surgery is as long as the list of procedures themselves. One study examined catheters that were inserted to deliver anesthetic into the epidural space around the spinal nerves for lower cesarean section, abdominal surgery, or prostate surgery. In some cases, non-sterile technique during catheter insertion resulted in serious infections, even leading to limb paralysis.(80)In one review of the literature, the authors found “a significant rate of overutilization of coronary angiography, coronary artery surgery, cardiac pacemaker insertion, upper gastrointestinal endoscopies, carotid endarterectomies, back surgery, and pain-relieving procedures.”(81)A 1987 JAMA study found the following significant levels of inappropriate surgery: 17% of coronary angiography procedures, 32% of carotid endarterectomy procedures, and 17% of upper gastrointestinal tract endoscopy procedures.(82) Based on the Healthcare Cost and Utilization Project (HCUP) statistics provided by the government for 2001, 697,675 upper gastrointestinal endoscopies (usually entailing biopsy) were performed, as were 142,401 endarterectomies and 719,949 coronary angiographies.(13) Extrapolating the JAMA study’s inappropriate surgery rates to 2001 produces 118,604 unnecessary endoscopy procedures, 45,568 unnecessary endarterectomies, and 122,391 unnecessary coronary angiographies. These are all forms of medical iatrogenesis.MEDICAL AND SURGICAL PROCEDURESIt is instructive to know the mortality rates associated with various medical and surgical procedures. Although we must sign release forms when we undergo any procedure, many of us are in denial about the true risks involved; because medical and surgical procedures are so commonplace, they often are seen as both necessary and safe. Unfortunately, allopathic medicine itself is a leading cause of death, as well as the most expensive way to die.Perhaps the words “health care” confer the illusion that medicine is about health. Allopathic medicine is not a purveyor of health care but of disease care. The HCUP figures are instructive,(13) but the computer program that calculates annual mortality statistics for all US hospital discharges is only as good as the codes entered into the system. In email correspondence, HCUP indicated that the mortality rates for each procedure indicated only that someone undergoing that procedure died either from the procedure or from some other cause.Thus there is no way of knowing exactly how many people die from a particular procedure. While codes for “poisoning & toxic effects of drugs” and “complications of treatment” do exist, the mortality figures registered in these categories are very low and do not correlate with what is known from research such as the 1998 JAMA study(1) that estimated an average of 106,000 prescription medication deaths per year. No codes exist for adverse drug side effects, surgical mishaps, or other types of medical error. Until such codes exist, the true mortality rates tied to of medical error will remain buried in the general statistics.AN HONEST LOOK AT U.S. HEALTH CAREIn 1978, the US Office of Technology Assessment (OTA) reported: “Only 10-20% of all procedures currently used in medical practice have been shown to be efficacious by controlled trial.”(83) In 1995, the OTA compared medical technology in eight countries ( Australia , Canada, France, Germany, the Netherlands, Sweden, the UK, and the US ) and again noted that few medical procedures in the US have been subjected to clinical trial. It also reported that US infant mortality was high and life expectancy low compared to other developed countries.(84)Although almost 10 years old, much of what was written in the OTA report holds true today. The report blames the high cost of American medicine on the medical free-enterprise system and failure to create a national health care policy. It attributes the government’s failure to control health care costs to market incentives and profit motives inherent in the current financing and organization of health care, which includes such interests as private health insurers, hospital systems, physicians, and the drug and medical-device industries. “Health Care Technology and Its Assessment in Eight Countries” is the last report prepared by the OTA, which was disbanded in 1995. It also is perhaps the US government’s last honest, detailed examination of the nation’s health care system. An appendix summarizing this 60-page report follows this article.SURGICAL ERRORS FINALLY REPORTEDAn October 2003 JAMA study from the US government’s Agency for Healthcare Research and Quality (AHRQ) documented 32,000 mostly surgery-related deaths costing $9 billion and accounting for 2.4 million extra hospital days in 2000.(85) Data from 20% of the nation’s hospitals were analyzed for 18 different surgical complications, including postoperative infections, foreign objects left in wounds, surgical wounds reopening, and post-operative bleeding.In a press release accompanying the study, AHRQ director Carolyn M. Clancy, MD, noted: “This study gives us the first direct evidence that medical injuries pose a real threat to the American public and increase the costs of health care.”(86) According to the study’s authors, “The findings greatly underestimate the problem, since many other complications happen that are not listed in hospital administrative data.” They added: “The message here is that medical injuries can have a devastating impact on the health care system. We need more research to identify why these injuries occur and find ways to prevent them from happening.” The study authors said that improved medical practices, including an emphasis on better hand washing, might help reduce morbidity and mortality rates. In an accompanying JAMA editorial, health-risk researcher Dr. Saul Weingart of Harvard’s Beth Israel-Deaconess Medical Center wrote, “Given their staggering magnitude, these estimates are clearly sobering.”(87)UNNECESSARY X-RAYSWhen x-rays were discovered, no one knew the long-term effects of ionizing radiation. In the 1950s, monthly fluoroscopic exams at the doctor’s office were routine, and you could even walk into most shoe stores and see x-rays of your foot bones. We still do not know the ultimate outcome of our initial fascination with x-rays.In those days, it was common practice to x-ray pregnant women to measure their pelvises and make a diagnosis of twins. Finally, a study of 700,000 children born between 1947 and 1964 in 37 major maternity hospitals compared the children of mothers who had received pelvic x-rays during pregnancy to those of mothers who did not. It found that cancer mortality was 40% higher among children whose mothers had been x-rayed.(88)In present-day medicine, coronary angiography is an invasive surgical procedure that involves snaking a tube through a blood vessel in the groin up to the heart. To obtain useful information, X-rays are taken almost continuously, with minimum dosages ranging from 460 to 1,580 mrem. The minimum radiation from a routine chest x-ray is 2 mrem. X-ray radiation accumulates in the body, and ionizing radiation used in X-ray procedures has been shown to cause gene mutation. The health impact of this high level of radiation is unknown, and often obscured in statistical jargon such as, “The risk for lifetime fatal cancer due to radiation exposure is estimated to be 4 in one million per 1,000 mrem.”(89)Dr. John Gofman has studied the effects of radiation on human health for 45 years. A medical doctor with a PhD in nuclear and physical chemistry, Gofman worked on the Manhattan Project, discovered uranium-233, and was the first person to isolate plutonium. In five scientifically documented books, Gofman provides strong evidence that medical technology—specifically x-rays, CT scans, and mammography and fluoroscopy devices—are a contributing factor to 75% of new cancers.In a nearly 700-page report updated in 2000, “Radiation from Medical Procedures in the Pathogenesis of Cancer and Ischemic Heart Disease: Dose-Response Studies with Physicians per 100,000 Population,”(90) Gofman shows that as the number of physicians increases in a geographical area along with an increase in the number of x-ray diagnostic tests performed, the rate of cancer and ischemic heart disease also increases. Gofman elaborates that it is not x-rays alone that cause the damage but a combination of health risk factors that include poor diet, smoking, abortions, and the use of birth control pills. Dr. Gofman predicts that ionizing radiation will be responsible for 100 million premature deaths over the next decade.In his book, Preventing Breast Cancer, Dr. Gofman notes that breast cancer is the leading cause of death among American women between the ages of 44 and 55. Because breast tissue is highly sensitive to radiation, mammograms can cause cancer. The danger can be heightened other factors including a woman’s genetic makeup, preexisting benign breast disease, artificial menopause, obesity, and hormonal imbalance.(91)Even x-rays for back pain can lead someone into crippling surgery. Dr. John E. Sarno, a well-known New York orthopedic surgeon, found that there is not necessarily any association between back pain and spinal x-ray abnormality. He cites studies of normal people without a trace of back pain whose x-rays indicate spinal abnormalities and of people with back pain whose spines appear to be normal on x-ray.(92) People who happen to have back pain and show an abnormality on x-ray may be treated surgically, sometimes with no change in back pain, worsening of back pain, or even permanent disability. Moreover, doctors often order x-rays as protection against malpractice claims, to give the impression of leaving no stone unturned. It appears that doctors are putting their own fears before the interests of their patients.UNNECESSARY HOSPITALIZATIONNearly 9 million (8,925,033) people were hospitalized unnecessarily in 2001.(4) In a study of inappropriate hospitalization, two doctors reviewed 1,132 medical records. They concluded that 23% of all admissions were inappropriate and an additional 17% could have been handled in outpatient clinics. Thirty-four percent of all hospital days were deemed inappropriate and could have been avoided.(93) The rate of inappropriate hospital admissions in 1990 was 23.5%.(94) In 1999, another study also found an inappropriate admissions rate of 24%, indicating a consistent pattern from 1986 to 1999.(95) The HCUP database indicates that the total number of patient discharges from US hospitals in 2001 was 37,187,641,(13) meaning that almost 9 million people were exposed to unnecessary medical intervention in hospitals and therefore represent almost 9 million potential iatrogenic episodes.(4)WOMEN’S EXPERIENCE IN MEDICINEDr. Martin Charcot (1825-1893) was world-renowned, the most celebrated doctor of his time. He practiced in the Paris hospital La Salpetriere. He became an expert in hysteria, diagnosing an average of 10 hysterical women each day, transforming them into “iatrogenic monsters” and turning simple “neurosis” into hysteria.(96) The number of women diagnosed with hysteria and hospitalized rose from 1% in 1841 to 17% in 1883. Hysteria is derived from the Latin “hystera” meaning uterus.According to Dr. Adriane Fugh-Berman, US medicine has a tradition of excessive medical and surgical interventions on women. Only 100 years ago, male doctors believed that female psychological imbalance originated in the uterus. When surgery to remove the uterus was perfected, it became the “cure” for mental instability, effecting a physical and psychological castration. Fugh-Berman notes that US doctors eventually disabused themselves of that notion but have continued to treat women very differently than they treat men.(97) She cites the following statistics:- Thousands of prophylactic mastectomies are performed annually.
- One-third of US women have had a hysterectomy before menopause.
- Women are prescribed drugs more frequently than are men.
- Women are given potent drugs for disease prevention, which results in disease substitution due to side effects.
- Fetal monitoring is unsupported by studies and not recommended by the CDC.(98) It confines women to a hospital bed and may result in a higher incidence of cesarean section.(99)
- Normal processes such as menopause and childbirth have been heavily “medicalized.”
- Synthetic hormone replacement therapy (HRT) does not prevent heart disease or dementia, but does increase the risk of breast cancer, heart disease, stroke, and gall bladder attack.(100)
As many as one-third of postmenopausal women use HRT.(101,102) This number is important in light of the much-publicized Women’s Health Initiative Study, which was halted before its completion because of a higher death rate in the synthetic estrogen-progestin (HRT) group.(103)CESAREAN SECTIONIn 1983, 809,000 cesarean sections (21% of live births) were performed in the US, making it the nation’s most common obstetric-gynecologic (OB/GYN) surgical procedure. The second most common OB/GYN operation was hysterectomy (673,000), followed by diagnostic dilation and curettage of the uterus (632,000). In 1983, OB/GYN procedures represented 23% of all surgery completed in the US.(104)In 2001, cesarean section is still the most common OB/GYN surgical procedure. Approximately 4 million births occur annually, with 24% (960,000) delivered by cesarean section. In the Netherlands, only 8% of births are delivered by cesarean section. This suggests 640,000 unnecessary cesarean sections—entailing three to four times higher mortality and 20 times greater morbidity than vaginal delivery(105)—are performed annually in the US.The US cesarean rate rose from just 4.5% in 1965 to 24.1% in 1986. Sakala contends that an “uncontrolled pandemic of medically unnecessary cesarean births is occurring.”(106) VanHam reported a cesarean section postpartum hemorrhage rate of 7%, a hematoma formation rate of 3.5%, a urinary tract infection rate of 3%, and a combined postoperative morbidity rate of 35.7% in a high-risk population undergoing cesarean section.(107)NEVER ENOUGH STUDIESScientists claimed there were never enough studies revealing the dangers of DDT and other dangerous pesticides to ban them. They also used this argument for tobacco, claiming that more studies were needed before they could be certain that tobacco really caused lung cancer. Even the American Medical Association (AMA) was complicit in suppressing the results of tobacco research. In 1964, when the Surgeon General’s report condemned smoking, the AMA refused to endorse it, claiming a need for more research. What they really wanted was more money, which they received from a consortium of tobacco companies that paid the AMA $18 million over the next nine years during which the AMA said nothing about the dangers of smoking.(108)The Journal of the American Medical Association (JAMA), “after careful consideration of the extent to which cigarettes were used by physicians in practice,” began accepting tobacco advertisements and money in 1933. State journals such as the New York State Journal of Medicine also began to run advertisements for Chesterfield cigarettes that claimed cigarettes are “Just as pure as the water you drink… and practically untouched by human hands.” In 1948, JAMA argued “more can be said in behalf of smoking as a form of escape from tension than against it… there does not seem to be any preponderance of evidence that would indicate the abolition of the use of tobacco as a substance contrary to the public health.”(109) Today, scientists continue to use the excuse that more studies are needed before they will support restricting the inordinate use of drugs.ADVERSE DRUG REACTIONSThe Lazarou study(1) analyzed records for prescribed medications for 33 million US hospital admissions in 1994. It discovered 2.2 million serious injuries due to prescribed drugs; 2.1% of inpatients experienced a serious adverse drug reaction, 4.7% of all hospital admissions were due to a serious adverse drug reaction, and fatal adverse drug reactions occurred in 0.19% of inpatients and 0.13% of admissions. The authors estimated that 106,000 deaths occur annually due to adverse drug reactions.Using a cost analysis from a 2000 study in which the increase in hospitalization costs per patient suffering an adverse drug reaction was $5,483, costs for the Lazarou study’s 2.2 million patients with serious drug reactions amounted to $12 billion.(1,49)Serious adverse drug reactions commonly emerge after FDA approval of the drugs involved. The safety of new agents cannot be known with certainty until a drug has been on the market for many years.(110)BEDSORESOver one million people develop bedsores in U.S. hospitals every year. It’s a tremendous burden to patients and family, and a $55 billion dollar healthcare burden. (7) Bedsores are preventable with proper nursing care. It is true that 50% of those affected are in a vulnerable age group of over 70. In the elderly bedsores carry a fourfold increase in the rate of death. The mortality rate in hospitals for patients with bedsores is between 23% and 37%. (8) Even if we just take the 50% of people over 70 with bedsores and the lowest mortality at 23%, that gives us a death rate due to bedsores of 115,000. Critics will say that it was the disease or advanced age that killed the patient, not the bedsore, but our argument is that an early death, by denying proper care, deserves to be counted. It is only after counting these unnecessary deaths that we can then turn our attention to fixing the problem.MALNUTRITION IN NURSING HOMESThe General Accounting Office (GAO), a special investigative branch of Congress, cited 20% of the nation’s 17,000 nursing homes for violations between July 2000 and January 2002. Many violations involved serious physical injury and death.(111)A report from the Coalition for Nursing Home Reform states that at least one-third of the nation’s 1.6 million nursing home residents may suffer from malnutrition and dehydration, which hastens their death. The report calls for adequate nursing staff to help feed patients who are not able to manage a food tray by themselves.(11) It is difficult to place a mortality rate on malnutrition and dehydration. The Coalition report states that malnourished residents, compared with well-nourished hospitalized nursing home residents, have a fivefold increase in mortality when they are admitted to a hospital. Multiplying the one-third of 1.6 million nursing home residents who are malnourished by a mortality rate of 20%(8,14) results in 108,800 premature deaths due to malnutrition in nursing homes.NOSOCOMIAL INFECTIONSThe rate of nosocomial infections per 1,000 patient days rose from 7.2 in 1975 to 9.8 in 1995, a 36% jump in 20 years. Reports from more than 270 US hospitals showed that the nosocomial infection rate itself had remained stable over the previous 20 years, with approximately five to six hospital-acquired infections occurring per 100 admissions, a rate of 5-6%. Due to progressively shorter inpatient stays and the increasing number of admissions, however, the number of infections increased. It is estimated that in 1995, nosocomial infections cost $4.5 billion and contributed to more than 88,000 deaths, or one death every 6 minutes.(9)The 2003 incidence of nosocomial mortality is quite probably higher than in 1995 because of the tremendous increase in antibiotic-resistant organisms. Morbidity and Mortality Report found that nosocomial infections cost $5 billion annually in 1999,(10) representing a $0.5 billion increase in just four years. At this rate of increase, the current cost of nosocomial infections would be around $5.5 billion.OUTPATIENT IATROGENESISIn a 2000 JAMA article, Dr. Barbara Starfield presents well-documented facts that are both shocking and unassailable.(12) The U.S. ranks 12th of 13 industrialized countries when judged by 16 health status indicators. Japan, Sweden, and Canada were first, second, and third, respectively. More than 40 million people in the US have no health insurance, and 20-30% of patients receive contraindicated care.Starfield warns that one cause of medical mistakes is overuse of technology, which may create a “cascade effect” leading to still more treatment. She urges the use of ICD (International Classification of Diseases) codes that have designations such as “Drugs, Medicinal, and Biological Substances Causing Adverse Effects in Therapeutic Use” and “Complications of Surgical and Medical Care” to help doctors quantify and recognize the magnitude of the medical error problem. Starfield notes that many deaths attributable to medical error today are likely to be coded to indicate some other cause of death. She concludes that against the backdrop of our poor health report card compared to other Westernized countries, we should recognize that the harmful effects of health care interventions account for a substantial proportion of our excess deaths.Starfield cites Weingart’s 2000 article, “Epidemiology of Medical Error,” as well as other authors to suggest that between 4% and 18% of consecutive patients in outpatient settings suffer an iatrogenic event leading to:1. 116 million extra physician visits2. 77 million extra prescriptions filled3. 17 million emergency department visits4. 8 million hospitalizations5. 3 million long-term admissions6. 199,000 additional deaths7. $77 billion in extra costs(112)UNNECESSARY SURGERIESWhile some 12,000 deaths occur each year from unnecessary surgeries, results from the few studies that have measured unnecessary surgery directly indicate that for some highly controversial operations, the proportion of unwarranted surgeries could be as high as 30%.(74)MEDICAL ERRORS: A GLOBAL ISSUEA five-country survey published in the Journal of Health Affairs found that 18-28% of people who were recently ill had suffered from a medical or drug error in the previous two years. The study surveyed 750 recently ill adults. The breakdown by country showed the percentages of those suffering a medical or drug error were 18% in Britain, 23% in Australia and in New Zealand, 25% in Canada, and 28% in the US.(113)HEALTH INSURANCEThe Institute of Medicine recently found that the 41 million Americans with no health insurance have consistently worse clinical outcomes than those who are insured, and are at increased risk for dying prematurely (114).When doctors bill for services they do not render, advise unnecessary tests, or screen everyone for a rare condition, they are committing insurance fraud. The US GAO estimated that $12 billion dollars was lost to fraudulent or unnecessary claims in 1998, and reclaimed $480 million in judgments in that year. In 2001, the federal government won or negotiated more than $1.7 billion in judgments, settlements, and administrative impositions in health care fraud cases and proceedings.(115)WAREHOUSING OUR ELDERSOne way to measure the moral and ethical fiber of a society is by how it treats its weakest and most vulnerable members. In some cultures, elderly people lives out their lives in extended family settings that enable them to continue participating in family and community affairs. American nursing homes, where millions of our elders go to live out their final days, represent the pinnacle of social isolation and medical abuse.- In America, approximately 1.6 million elderly are confined to nursing homes. By 2050, that number could be 6.6 million.(11,116)
- Twenty percent of all deaths from all causes occur in nursing homes.(117)
- Hip fractures are the single greatest reason for nursing home admissions.(118)
- Nursing homes represent a reservoir for drug-resistant organisms due to overuse of antibiotics.(119)
Presenting a report he sponsored entitled “Abuse of Residents is a Major Problem in U.S. Nursing Homes” on July 30, 2001, Rep. Henry Waxman (D-CA) noted that “as a society we will be judged by how we treat the elderly.” The report found one-third of the nation’s approximately 17,000 nursing homes were cited for an abuse violation in a two-year period from January 1999 to January 2001.(116) According to Waxman, “the people who cared for us deserve better.” The report suggests that this known abuse represents only the “tip of the iceberg” and that much more abuse occurs that we aware of or ignore.(116a) The report found:- Over 30% of US nursing homes were cited for abuses, totaling more than 9,000 violations.
- 10% of nursing homes had violations that caused actual physical harm to residents or worse.
- Over 40% (3,800) of the abuse violations followed the filing of a formal complaint, usually by concerned family members.
- Many verbal abuse violations were found.
- Occasions of sexual abuse.
- Incidents of physical abuse causing numerous injuries such as fractured femur, hip, elbow, wrist, and other injuries.
Dangerously understaffed nursing homes lead to neglect, abuse, overuse of medications, and physical restraints. In 1990, Congress mandated an exhaustive study of nurse-to-patient ratios in nursing homes. The study was finally begun in 1998 and took four years to complete.(120) A spokesperson for The National Citizens’ Coalition for Nursing Home Reform commented on the study: “They compiled two reports of three volumes each thoroughly documenting the number of hours of care residents must receive from nurses and nursing assistants to avoid painful, even dangerous, conditions such as bedsores and infections. Yet it took the Department of Health and Human Services and Secretary Tommy Thompson only four months to dismiss the report as ‘insufficient.’”(121) Although preventable with proper nursing care, bedsores occur three times more commonly in nursing homes than in acute care or veterans hospitals.(122).Because many nursing home patients suffer from chronic debilitating conditions, their assumed cause of death often is unquestioned by physicians. Some studies show that as many as 50% of deaths due to restraints, falls, suicide, homicide, and choking in nursing homes may be covered up.(123,124) It is possible that many nursing home deaths are instead attributed to heart disease. In fact, researchers have found that heart disease may be over-represented in the general population as a cause of death on death certificates by 8-24%. In the elderly, the overreporting of heart disease as a cause of death is as much as twofold.(125)That very few statistics exist concerning malnutrition in acute-care hospitals and nursing homes demonstrates the lack of concern in this area. While a survey of the literature turns up few US studies, one revealing US study evaluated the nutritional status of 837 patients in a 100-bed subacute-care hospital over a 14-month period. The study found only 8% of the patients were well nourished, while 29% were malnourished and 63% were at risk of malnutrition. As a result, 25% of the malnourished patients required readmission to an acute-care hospital, compared to 11% of the well-nourished patients. The authors concluded that malnutrition reached epidemic proportions in patients admitted to this subacute-care facility.(126)Many studies conclude that physical restraints are an underreported and preventable cause of death. Studies show that compared to no restraints, the use of restraints carries a higher mortality rate and economic burden.(127-129) Studies have found that physical restraints, including bedrails, are the cause of at least 1 in every 1,000 nursing-home deaths.(130-132)Deaths caused by malnutrition, dehydration, and physical restraints, however, are rarely recorded on death certificates. Several studies reveal that nearly half of the listed causes of death on death certificates for elderly people with chronic or multi-system disease are inaccurate.(133) Even though 1 in 5 people die in nursing homes, an autopsy is performed in less than 1% of these deaths.(134).OVERMEDICATING SENIORSDr. Robert Epstein, chief medical officer of Medco Health Solutions Inc. (a unit of Merck & Co.), conducted a study in 2003 of drug trends among the elderly.(135) He found that seniors are going to multiple physicians, getting multiple prescriptions, and using multiple pharmacies. Medco oversees drug-benefit plans for more than 60 million Americans, including 6.3 million seniors who received more than 160 million prescriptions. According to the study, the average senior receives 25 prescriptions each year. Among those 6.3 million seniors, a total of 7.9 million medication alerts were triggered: less than one-half that number, 3.4 million, were detected in 1999.About 2.2 million of those alerts indicated excessive dosages unsuitable for seniors, and about 2.4 million alerts indicated clinically inappropriate drugs for the elderly. Reuters interviewed Kasey Thompson, director of the Center on Patient Safety at the American Society of Health System Pharmacists, who noted: “There are serious and systemic problems with poor continuity of care in the United States .” He says this study represents only “the tip of the iceberg” of a national problem.According to Drug Benefit Trends , the average number of prescriptions dispensed per non-Medicare HMO member per year rose 5.6% from 1999 to 2000, – from 7.1 to 7.5 prescriptions. The average number dispensed for Medicare members increased 5.5%, from 18.1 to 19.1 prescriptions.(136) The total number of prescriptions written in the US in 2000 was 2.98 billion, or 10.4 prescriptions for every man, woman, and child.(137)In a study of 818 residents of residential care facilities for the elderly, 94% were receiving at least one medication at the time of the interview. The average intake of medications was five per resident; the authors noted that many of these drugs were given without a documented diagnosis justifying their use.(138)Seniors and groups like the American Association for Retired Persons (AARP) are demanding that prescription drug coverage be a basic right.(139) They have accepted allopathic medicine’s overriding assumption that aging and dying in America must be accompanied by drugs in nursing homes and eventual hospitalization. Seniors are given the choice of either high-cost patented drugs or low-cost generic drugs. Drug companies attempt to keep the most expensive drugs on the shelves and suppress access to generic drugs, despite facing stiff fines of hundreds of millions of dollars levied by the federal government.(140,141) In 2001, some of the world’s largest drug companies were fined a record $871 million for conspiring to increase the price of vitamins.(142)Current AARP recommendations for diet and nutrition assume that seniors are getting all the nutrition they need in an average diet. At most, AARP suggests adding extra calcium and a multivitamin and mineral supplement.(143)Ironically, studies also indicate underuse of proper pain medication for patients who need it. One study evaluated pain management in a group of 13,625 cancer patients, aged 65 and over, living in nursing homes. While almost 30% of the patients reported pain, more than 25% received no pain relief medication, 16% received a mild analgesic drug, 32% received a moderate analgesic drug, and 26% received adequate pain-relieving morphine. The authors concluded that older patients and minority patients were more likely to have their pain untreated.(144)WHAT REMAINS TO BE UNCOVEREDOur ongoing research will continue to quantify the morbidity, mortality, and financial loss due to:1. X-ray exposures (mammography, fluoroscopy, CT scans).2. Overuse of antibiotics for all conditions.3. Carcinogenic drugs (hormone replacement therapy,* immunosuppressive and prescription drugs).4. Cancer chemotherapy(70)5. Surgery and unnecessary surgery (cesarean section, radical mastectomy, preventive mastectomy, radical hysterectomy, prostatectomy, cholecystectomies, cosmetic surgery, arthroscopy, etc.).6. Discredited medical procedures and therapies.7. Unproven medical therapies.8. Outpatient surgery.9. Doctors themselves.* Part of our ongoing research will be to quantify the mortality and morbidity caused by hormone replacement therapy (HRT) since the 1940s. In December 2000, a government scientific advisory panel recommended that synthetic estrogen be added to the nation’s list of cancer-causing agents. HRT, either synthetic estrogen alone or combined with synthetic progesterone, is used by an estimated 13.5 to 16 million women in the US.(145) The aborted Women’s Health Initiative Study (WHI) of 2002 showed that women taking synthetic estrogen combined with synthetic progesterone have a higher incidence of ovarian cancer, breast cancer, stroke, and heart disease, with little evidence of osteoporosis reduction or dementia prevention. WHI researchers, who usually never make recommendations except to suggest more studies, advised doctors to be very cautious about prescribing HRT to their patients.(100,146-150)Results of the “Million Women Study” on HRT and breast cancer in the UK were published in medical journal The Lancet in August 2003. According to lead author Prof. Valerie Beral, director of the Cancer Research UK Epidemiology Unit: “We estimate that over the past decade, use of HRT by UK women aged 50-64 has resulted in an extra 20,000 breast cancers, estrogen-progestagen (combination) therapy accounting for 15,000 of these.”(151) We were unable to find statistics on breast cancer, stroke, uterine cancer, or heart disease caused by HRT used by American women. Because the US population is roughly six times that of the UK, it is possible that 120,000 cases of breast cancer have been caused by HRT in the past decade.OFFICE OF TECHNOLOGY ASSESSMENT (OTA)Health Care Technology and Its Assessment in Eight Countries, 1995.General Facts1. In 1990, US life expectancy was 71.8 years for men and 78.8 years for women, among the lowest rates in the developed countries.2. The 1990 US infant mortality rate in the US was 9.2 per 1,000 live births, in the bottom half of the distribution among all developed countries.3. Health status is correlated with socioeconomic status.4. Health care is not universal.5. Health care is based on the free market system with no fixed budget or limitations on expansion.6. Health care accounts for 14% of the US GNP ($800 billion in 1993).7. The federal government does no central planning, though it is the major purchaser of health care for older people and some poor people.8. Americans are less satisfied with their health care system than people in other developed countries.9. US medicine specializes in expensive medical technology; some large US cities have more magnetic resonance image (MRI) scanners than most countries.10. Huge public and private investments in medical research and pharmaceutical development drive this “technological arms race.”11. Any efforts to restrain technological developments in health care are opposed by policymakers concerned about negative impacts on medical-technology industries.Hospitals1. In 1990, the US had 5,480 acute-care hospitals, 880 specialty (psychiatric, long-term care, and rehabilitation) hospitals, and 340 federal (military, veterans, and Native American) hospitals, or 2.7 hospitals per 100,000 population.2. In 1990, the average length of stay for 33 million admissions was 9.2 days. The bed occupancy rate was 66%. Lengths of stay were shorter and admission rates lower than other countries.3. In 1990, the US had 615,000 physicians, or 2.4 per 1,000 population; 33% were primary care (family medicine, internal medicine, and pediatrics) and 67% were specialists.4. In 1991, government-run health care spending totaled $81 billion.5. Total US health care spending rose to $752 billion in 1991 from $70 billion in 1950. Spending grew five-fold per capita.6. Reasons for increased healthcare spending include:1. The high cost of defensive medicine, with an escalation in services solely to avoid malpractice litigation.2. US health care based on defensive medicine costs nearly $45 billion per year, or about 5% of total health care spending, according to one source.3. The availability and use of new medical technologies have contributed the most to increased health care spending, argue many analysts. These costs are impossible to quantify.7. The reasons government attempts to control health care costs have failed include:1. Market incentive and profit-motive involvement in the financing and organization of health care, including private insurers, hospital systems, physicians, and the drug and medical-device industries.2. Expansion is the goal of free enterprise.Health-Related Research and Development1. The US spends more than any other country on health-related R&D.2. In 1989, the federal government spent $9.2 billion on R&D, while private industry spent an additional $9.4 billion.3. Total US R&D expenditures rose 50% from 1983 to 1992.4. NIH receives about half of US government R&D funding.5. NIH spent more on basic research ($4.1 billion in 1989) than for clinical trials of medical treatments on humans ($519 million in 1989).6. Most of the clinical trials evaluate new treatment protocols for cancer and complications of AIDS, and do not study existing treatments, even though their effectiveness is in many cases unknown and questionable.7. In 1990, the NIH had just begun to do meta-analysis and cost-effectiveness analysis.Pharmaceutical and Medical-Device Industries1. About two-thirds of the industry’s $9.4 billion budget went to drug research; device manufacturers spent the remaining one-third.2. In addition to R&D, the medical industry spent 24% of total sales on promoting their products and 15% of total sales on development.3. Total marketing expenses in 1990 were over $5 billion.4. Many products provide no benefit over existing products.5. Public and private health care consumers buy these products.6. If health care spending is perceived as a problem, a highly profitable drug industry exacerbates the problem.Controlling Health Care Technology1. The FDA ensures the safety and efficacy of drugs, biologics, and medical devices.2. The FDA does not consider costs of therapy.3. The FDA does not consider the effectiveness of a therapy.4. The FDA does not compare a product to currently marketed products5. The FDA does not consider nondrug alternatives for a given clinical problem.6. It costs $200 million in development costs to bring a new drug to market. AIDS-drug interest groups forced new regulations that speed up the approval process.7. Such drugs should be subject to greater post-marketing surveillance requirements. As of 1995, these provisions had not yet come into play.8. Many argue that reductions in the pre-approval testing of drugs open the possibility of significant undiscovered toxicities.Health Care Technology Assessment1. Failure to evaluate technology was a focus of a 1978 report from OTA with examples of many common medical practices supported by limited published data (10-20%).2. In 1978, Congress created the National Center for Health Care Technology (NCHCT) to advise Medicare and Medicaid.3. With an annual budget of $4 million, NCHCT published three broad assessments of high-priority technologies and made about 75 coverage recommendations to Medicare.4. Congress disbanded NCHCT in 1981. The medical profession opposed it from the beginning. The AMA testified before Congress in 1981 that “clinical policy analysis and judgments are better made—and are being responsibly made—within the medical profession. Assessing risks and costs, as well as benefits, has been central to the exercise of good medical judgment for decades.”5. The medical device lobby also opposed government oversight by NCHCT.Examples of Lack of Proper Management of HealthCareTreatments for Coronary Artery Disease1. Since the early 1970s, the number of coronary artery bypass surgeries (CABGS) has risen rapidly without government regulation or clinical trials.2.Angioplastyforsinglevesseldiseasewasintroducedin1978Thefirstpublishedtrialofangioplastyversus
medical treatment was done in 1992.3. Angioplasty did not reduce the number of CABGS, as was promoted.4. Both procedures increase in number every year as the patient population grows older and sicker.5. Rates of use are higher in white patients and private insurance patients, and vary greatly by geographic region, suggesting that use of these procedures is based on non-clinical factors.6. As of 1995, the NIH consensus program had not assessed CABGS since 1980 and had never assessed angioplasty.7. RAND researchers evaluated CABGS in New York in 1990. They reviewed 1,300 procedures and found 2% were inappropriate, 90% were appropriate, and 7% were uncertain. For 1,300 angioplasties, 4% were inappropriate and 38% uncertain. Using RAND methodologies, a panel of British physicians rated twice as many procedures “inappropriate” as did a US panel rating the same clinical cases. The New York numbers are in question because New York State limits the number of surgery centers, and the per-capita supply of cardiac surgeons in New York is about one-half of the national average.8. The estimated five-year cost is $33,000 for angioplasty and $40,000 for CABGS. Angioplasty did not lower costs, due to its high failure rates.Computed Tomography (CT)1. The first CT scanner in the US was installed at the Mayo Clinic in 1973. By 1992, the number of operational CT scanners in the US had grown to 6,060. By comparison, in 1993 there were 216 CT units in Canada .2. There is little information available on how CT scans improve or affect patient outcomes3. In some institutions, up to 90% of scans performed were negative.4. Approval by the FDA was not required for CT scanners, nor was any evidence of safety or efficacy.Magnetic Resonance Imaging (MRI)1. MRIs were introduced in Great Britain in 1978 and in the US in 1980. By 1988, there were 1,230 units and by 1992 between 2,800 and 3,000.2. A definitive review published in 1994 found less than 30 studies of 5,000 that were prospective comparisons of diagnostic accuracy or therapeutic choice.3. The American College of Physicians assessed MRI studies and rated 13 of 17 trials as “weak,” i.e., lacking data concerning therapeutic impact or patient outcomes.4. The OTA concluded: “It is evident that hospitals, physician-entrepreneurs, and medical device manufacturers have approached MRI and CT as commodities with high-profit potential, and decision-making on the acquisition and use of these procedures has been highly influenced by this approach. Clinical evaluation, appropriate patient selection, and matching supply to legitimate demand might be viewed as secondary forces.”Laparoscopic Surgery1. Laparoscopic cholecystectomy was introduced at a professional surgical society meeting in late 1989. By 1992, 85% of all cholecystectomies were performed laparoscopically.2. There was an associated increase of 30% in the number of cholecystectomies performed.3. Because of the increased volume of gall bladder operations, their total cost increased 11.4% between 1988 and 1992, despite a 25.1% drop in the average cost per surgery.4. The mortality rate for gall bladder surgeries did not decline as a result of the lower risk because so many more were performed.5. When studies were finally done on completed cases, the results showed that laparoscopic cholecystectomy was associated with reduced inpatient duration, decreased pain, and a shorter period of restricted activity. But rates of bile duct and major vessel injury increased and it was suggested that these rates were worse for people with acute cholecystitis. No clinical trials had been done to clarify this issue.6. Patient demand, fueled by substantial media attention, was a major force in promoting rapid adoption of these procedures.7. The major manufacturer of laparoscopic equipment produced the video that introduced the procedure in 1989.8. Doctors were given two-day training seminars before performing the surgery on patients.Infant Mortality1. In 1990, the US ranked 24th in infant mortality of 38 developed countries with a rate of 9.2 deaths per 1,000 live births.2. US black infant mortality is 18.6 per 1,000 live births, compared to 8.8 for whites.Screening for Breast Cancer1. Mammography screening in women under 50 has always been a subject of debate.2. In 1992, the Canadian National Breast Cancer Study of 50,000 women showed that mammography had no effect on mortality for women aged 40-50.3. The National Cancer Institute (NCI) refused to change its recommendations on mammography.4. The American Cancer Society decided to wait for more studies on mammography.5. In December 1993, NCI announced that women over 50 should have routine screenings every one to two years but that younger women would derive no benefit from mammography.Summary1. The OTA concluded: “There are no mechanisms in place to limit dissemination of technologies regardless of their clinical value.” Shortly after the release of this report, the OTA was disbanded.
ALTERNATIVESPrevention is always better than cure. Do what we do; get toxins out of your life and study natural health.Learn natural health technologies that help to heal people, such as Applied Kinesiology.——-DOWNLOAD THIS ARTICLE AS A PDF Download——–RELATED ARTICLES———-REFERENCES1. Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA . 1998 Apr 15;279(15):1200-5.
2. Rabin R. Caution about overuse of antibiotics. Newsday . September 18, 2003 . 2a. Centers for Disease Control and Prevention. CDC antimicrobial resistance and antibiotic resistance—general information. Available at: http://www.cdc.gov/drugresistance/community/. Accessed December 13, 2003 .
3. For calculations detail, see “Unnecessary Surgery.” Sources: HCUPnet, Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality, Rockville , MD. Available at: http://www.ahrq.gov/data/hcup/hcupnet.htm . Accessed December 18, 2003 . US Congressional House Subcommittee Oversight Investigation. Cost and Quality of Health Care: Unnecessary Surgery . Washington , DC : Government Printing Office;1976. Cited in: McClelland GB, Foundation for Chiropractic Education and Research. Testimony to the Department of Veterans Affairs’ Chiropractic Advisory Committee. March 25, 2003 .
4. For calculations detail, see “Unnecessary Hospitalization.” Sources: HCUPnet, Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality, Rockville , MD. Available at: http://www.ahrq.gov/data/hcup/hcupnet.htm . Accessed December 18, 2003 . Siu AL, Sonnenberg FA, Manning WG, et al. Inappropriate use of hospitals in a randomized trial of health insurance plans. N Engl J Med . 1986 Nov 13;315(20):1259-66. Siu AL, Manning WG, Benjamin B. Patient, provider and hospital characteristics associated with inappropriate hospitalization. Am J Public Health . 1990 Oct;80(10):1253-6. Eriksen BO, Kristiansen IS, Nord E, et al. The cost of inappropriate admissions: a study of health benefits and resource utilization in a department of internal medicine. J Intern Med . 1999 Oct;246(4):379-87.
5. U.S. National Center for Health Statistics. National Vital Statistics Report, vol. 51, no. 5, March 14, 2003 .
6. Thomas, EJ, Studdert DM, Burstin HR, et al. Incidence and types of adverse events and negligent care in Utah and Colorado. Med Care. 2000 Mar;38(3):261-71. Thomas, EJ, Studdert DM, Newhouse JP, et al. Costs of medical injuries in Utah and Colorado . Inquiry . 1999 Fall;36(3):255-64. [Two references.] 7. Xakellis GC, Frantz R, Lewis A. Cost of pressure ulcer prevention in long-term care. Am Geriatr Soc . 1995 May;43(5):496-501.
8. Barczak CA, Barnett RI, Childs EJ, Bosley LM. Fourth national pressure ulcer prevalence survey. Adv Wound Care . 1997 Jul-Aug;10(4):18-26.
9. Weinstein RA. Nosocomial Infection Update. Emerg Infect Dis . 1998 Jul-Sep;4(3):416-20.
10. Fourth Decennial International Conference on Nosocomial and Healthcare-Associated Infections. Morbidity and Mortality Weekly Report. February 25, 2000 , Vol. 49, No. 7, p.138.
11. Burger SG, Kayser-Jones J, Bell JP. Malnutrition and dehydration in nursing homes: key issues in prevention and treatment. National Citizens’ Coalition for Nursing Home Reform. June 2000. Available at: http://www.cmwf.org/programs/elders/burger_mal_386.asp. Accessed December 13, 2003 .
12. Starfield B. Is US health really the best in the world? JAMA . 2000 Jul 26;284(4):483-5. Starfield B. Deficiencies in US medical care. JAMA . 2000 Nov 1;284(17):2184-5.
13. HCUPnet, Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality, Rockville , MD. Available at: http://www.ahrq.gov/data/hcup/hcupnet.htm . Accessed December 18, 2003 .
14. Nationwide poll on patient safety: 100 million Americans see medical mistakes directly touching them [press release]. McLean , VA : National Patient Safety Foundation; October 9, 1997 .
15. The Society of Actuaries Health Benefit Systems Practice Advancement Committee. The Troubled Healthcare System in the US . September 13, 2003 . Available at: http://www.soa.org/sections/troubled_healthcare.pdf. Accessed December 18, 2003 .
16. Leape LL. Error in medicine. JAMA . 1994 Dec 21;272(23):1851-7.
17. a.Brennan TA, Leape LL, Laird NM , et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med . 1991 Feb 7;324(6):370-6.
18. Campbell EG, Weissman JS, Clarridge B, Yucel R, Causino N, Blumenthal D. Characteristics of medical school faculty members serving on institutional review boards: results of a national survey. Acad Med . 2003 Aug;78(8):831-6.
19. Possible conflict of interest within medical profession. HealthDayNews. August 15, 2003 .
20. World Health Organization. Press Release Bulletin #9. December 17, 2001 .
21. Angell M. Is academic medicine for sale? N Engl J Med . 2000 May 18;342(20):1516-8.
22. McKenzie J. Conflict of interest? Medical journal changes policy of finding independent doctors [transcript]. ABC News. June 12, 2002 .
23. Crossen C. Tainted Truth: The Manipulation of Fact in America . New York , NY : Simon & Schuster; 1994.
24. Bates DW, Cullen DJ, Laird N, et al. Incidence of adverse drug events and potential adverse drug events. Implications for prevention. ADE Prevention Study Group. JAMA . 1995 Jul 5;274(1):29-34.
25. Vincent C, Stanhope N, Crowley-Murphy M. Reasons for not reporting adverse incidents: an empirical study. J Eval Clin Pract . 1999 Feb;5(1):13-21.
26. Wald H, Shojania KG. Incident reporting. In: Shojania KG, Duncan BW, McDonald KM, et al, eds. Making Health Care Safer: A Critical Analysis of Patient Safety Practices . Rockville , MD : Agency for Healthcare Research and Quality; 2001:chap 4. Evidence Report/Technology Assessment No. 43. AHRQ publication 01-E058.
27. Grinfeld MJ. The debate over medical error reporting. Psychiatric Times . April 2000.
28. King G III, Hermodson A. Peer reporting of coworker wrongdoing: A qualitative analysis of observer attitudes in the decision to report versus not report unethical behavior. Journal of Applied Communication Research . 2000;(28), 309-29.
29. Gilman AG, Rall TW, Nies AS , Taylor P. Goodman and Gilman’s The Pharmacological Basis of Therapeutics. New York , NY : Pergamon Press; 1996.
30. Kolata G. New York Times News Service. Who cares when our drugs fail? San Diego Union-Tribune . October 15, 1997 :E-1,5.
31. Melmon KL, Morrelli HF, Hoffman BB, Nierenberg DW, eds. Melmon and Morrelli’s Clinical Pharmacology: Basic Principles in Therapeutics . 3rd ed. New York , NY : McGraw-Hill, Inc., 1992.
32. Moore TJ, Psaty BM, Furberg CD. Time to act on drug safety . JAMA . 1998 May 20, 279 (19):1571-3. 32 a.Cullen DJ, Bates DW, Small SD, Cooper JB, Nemeskal AR , Leape LL. The incident reporting system does not detect adverse drug events: a problem for quality improvement. Jt Comm J Qual Improv . 1995 Oct;21(10):541-8.
33. Bates DW. Drugs and adverse drug reactions: how worried should we be? JAMA . 1998 Apr 15;279(15):1216-7.
34. Dickinson, JG. FDA seeks to double effort on confusing drug names. Dickinson ‘s FDA Review . 2000 Mar;7(3):13-4.
35. Cohen JS. Overdose: The Case Against the Drug Companies . New York , NY : Tarcher-Putnum; 2001.
36. Stenson J. Few residents report medical errors, survey finds. Reuters Health. February 21, 2003 .
37. Survey by Henry J. Kaiser Family Foundation, Harvard School of Public Health. Methodology: Fieldwork conducted by ICR – International Communications Research, April 11- June 11, 2002
38. Bond CA, Raehl CL, Franke T. Clinical pharmacy services, hospital pharmacy staffing, and medication errors in United States hospitals. Pharmacotherapy . 2002 Feb;22(2):134-47.
39. Barker KN, Flynn EA, Pepper GA, Bates DW, Mikeal RL. Medication errors observed in 36 health care facilities. Arch Intern Med . 2002 Sep 9;162(16):1897-903.
40. LaPointe NM , Jollis JG. Medication errors in hospitalized cardiovascular patients. Arch Intern Med . 2003 Jun 23;163(12):1461-6.
41. Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med . 2003 Feb 4;138(3):161-7.
42. Gandhi TK, Weingart SN, Borus J, et al. Adverse drug events in ambulatory care. N Engl J Med . 2003 Apr 17;348(16):1556-64.
43. Medication side effects strike 1 in 4. Reuters. April 17, 2003 .
44. Vastag B. Pay attention: ritalin acts much like cocaine. JAMA . 2001 Aug 22-29;286(8):905-6.
45. Rosenthal MB, Berndt ER, Donohue JM, Frank RG, Epstein AM. Promotion of prescription drugs to consumers. N Engl J Med . 2002 Feb 14;346(7):498-505.
46. Wolfe SM. Direct-to-consumer advertising—education or emotion promotion? N Engl J Med . 2002 Feb 14;346(7):524-6.
47. Ibid.
48. US General Accounting Office. Report to the Chairman, Subcommittee on Human Resources and Intergovernmental Relations, Committee on Government Operations, House of Representatives: FDA Drug Review Postapproval Risks 1976-85 . Washington , DC : US General Accounting Office; 1990:3.
49. Drug giant accused of false claims. MSNBC News. July 11, 2003 . Available at: http://msnbc.com/news/937302.asp?0sl=-42&cp1=1. Accessed December 17,2003 .
50. Suh DC , Woodall BS, Shin SK , Hermes-De Santis ER. Clinical and economic impact of adverse drug reactions in hospitalized patients. Ann Pharmacother . 2000 Dec;34(12):1373-9.
51. Agger WA. Antibiotic resistance: unnatural selection in the office and on the farm. Wisconsin Medical Journal . August 2002.
52. Nash DR, Harman J, Wald ER, Kelleher KJ. Antibiotic prescribing by primary care physicians for children with upper respiratory tract infections. Arch Pediatr Adolesc Med . 2002 Nov;156(11):1114-9.
53. Schindler C, Krappweis J, Morgenstern I, Kirch W. Prescriptions of systemic antibiotics for children in Germany aged between 0 and 6 years. Pharmacoepidemiol Drug Saf . 2003 Mar;12(2):113-20.
54. Finkelstein JA, Stille C, Nordin J, et al. Reduction in antibiotic use among US children, 1996-2000. Pediatrics . 2003 Sep;112(3 Pt 1):620-7.
55. Linder JA, Stafford RS. Antibiotic treatment of adults with sore throat by community primary care physicians: a national survey, 1989-1999. JAMA . 2001 Sep 12;286(10):1181-6.
56. Drug resistance page. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/drugresistance/community/. Accessed December 17, 2003 .
57. Available at: http://www.health.state.ok.us/program/cdd/ar/. Accessed December 17, 2003 .
58. Available at: http://www.librainitiative.com/life/en/libra_initiative.html. Accessed December 17, 2003 .
59. Ohlsen K, Ternes T, Werner G, et al. Impact of antibiotics on conjugational resistance gene transfer in Staphylococcus aureus in sewage. Environ Microbiol . 2003 Aug;5(8):711-6.
60. Pawlowski S, Ternes T, Bonerz M, et al. Combined in situ and in vitro assessment of the estrogenic activity of sewage and surface water samples. Toxicol Sci . 2003 Sep;75(1):57-65. Epub 2003 Jun 12.
61. Ternes TA, Stuber J, Herrmann N, et al. Ozonation: a tool for removal of pharmaceuticals, contrast media and musk fragrances from wastewater? Water Res . 2003 Apr;37(8):1976-82.
62. Ternes TA, Meisenheimer M, McDowell D, et al. Removal of pharmaceuticals during drinking water treatment. Environ Sci Technol . 2002 Sep 1;36(17):3855-63.
63. Ternes T, Bonerz M, Schmidt T. Determination of neutral pharmaceuticals in wastewater and rivers by liquid chromatography-electrospray tandem mass spectrometry. J Chromatogr A . 2001 Dec 14;938(1-2):175-85.
64. Golet EM, Alder AC, Hartmann A, Ternes TA, Giger W. Trace determination of fluoroquinolone antibacterial agents in urban wastewater by solid-phase extraction and liquid chromatography with fluorescence detection. Anal Chem . 2001 Aug 1;73(15):3632-8.
65DhtCGTTAPhtildldtithittfbtlh?EiHlth
Perspect . 1999 Dec;107 Suppl 6:907-38.
66. Hirsch R, Ternes T, Haberer K, Kratz KL. Occurrence of antibiotics in the aquatic environment. Sci Total Environ . 1999 Jan 12;225(1-2):109-18.
67. Ternes TA, Stumpf M, Mueller J, Haberer K, Wilken RD , Servos M. Behavior and occurrence of estrogens in municipal sewage treatment plants—I. Investigations in Germany , Canada and Brazil . Sci Total Environ . 1999 Jan 12;225(1-2):81-90.
68. Hirsch R, Ternes TA, Haberer K, Mehlich A, Ballwanz F, Kratz KL. Determination of antibiotics in different water compartments via liquid chromatography-electrospray tandem mass spectrometry. J Chromatogr A . 1998 Jul 31;815(2):213-23.
69. Coste J, Hanotin C, Leutenegger E. Prescription of non-steroidal anti-inflammatory agents and risk of iatrogenic adverse effects: a survey of 1072 French general practitioners. Therapie . 1995 May-Jun;50(3):265-70.
70. Kouyanou K, Pither CE, Wessely S. Iatrogenic factors and chronic pain. Psychosom Med . 1997 Nov-Dec;59(6):597-604.
71. Abel U. Chemotherapy of advanced epithelial cancer—a critical review. Biomed Pharmacother . 1992;46(10):439-52.
72. Schulman KA, Stadtmauer EA, Reed SD , et al. Economic analysis of conventional-dose chemotherapy compared with high-dose chemotherapy plus autologous hematopoietic stem-cell transplantation for metastatic breast cancer. Bone Marrow Transplant . 2003 Feb;31(3):205-10.
73. Kaufman, M. Drugmaker to pay FDA $500 million. Manufacturing problems found at schering-plough . The Washington Post . May 18, 2002 :A01.
74. US Congressional House Subcommittee Oversight Investigation. Cost and Quality of Health Care: Unnecessary Surgery . Washington , DC : Government Printing Office;1976. Cited in: McClelland GB, Foundation for Chiropractic Education and Research. Testimony to the Department of Veterans Affairs’ Chiropractic Advisory Committee. March 25, 2003 .
75. Leape LL. Unnecessary surgery. Health Serv Res . 1989 Aug;24(3):351-407.
76. McClelland GB, Foundation for Chiropractic Education and Research. Testimony to the Department of Veterans Affairs’ Chiropractic Advisory Committee. March 25, 2003 .
77. Coile RC Jr. Internet-driven surgery. Russ Coiles Health Trends . 2003 Jun;15(8):2-4.
78. Guarner V. Unnecessary operations in the exercise of surgery. A topic of our times with serious implications in medical ethics. Gac Med Mex . 2000 Mar-Apr;136(2):183-8.
79. Rutkow IM. Surgical operations in the United States : 1979 to 1984. Surgery . 1987 Feb;101(2):192-200.
80. Rutkow IM. Surgical operations in the United States . Then (1983) and now (1994). Arch Surg . 1997 Sep;132(9):983-90.
81. Linnemann MU, Bulow HH. Infections after insertion of epidural catheters. Ugeskr Laeger . 1993 Jul 26;155(30):2350-2
82. Seres JL, Newman RI . Perspectives on surgical indications. Implications for controls. Clin J Pain . 1989 Jun;5(2):131-6.
83. Chassin MR, Kosecoff J, Park RE, et al. Does inappropriate use explain geographic variations in the use of health care services? A study of three procedures. JAMA. 1987 Nov 13;258(18):2533-7.
84. Office of Technology Assessment, US Congress. Assessing the Efficacy and Safety of Medical Technologies. Washington DC : Office of Technology Assessment, US Congress; 1978.
85. Tunis SR, Gelband H. Health care technology in the United States . Health Policy . 1994 Oct-Dec;30(1-3):335-96.
86. Zhan C, Miller M. Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization. JAMA . 2003;290:1868-1874.
87. Injuries in hospitals pose a significant threat to patients and a substantial increase in health care charges [press release]. Rockville , MD : Agency for Healthcare Research and Quality. October 7, 2003 . http://www.ahrq.gov/news/ress/pr2003/injurypr.htm.
88. Weingart SN, Iezzoni LI. Looking for medical injuries where the light is bright. JAMA . 2003 Oct 8 ;290(14):1917-9.
89. MacMahon B. Prenatal x-ray exposure and childhood cancer. J Natl Cancer Inst . 1962 May;28:1173-91.
90. Health Physics Society. Available at: http://hps.org/publicinformation/ate/q1084.html. Accessed December 17, 2003 .
91. Gofman JW. Radiation from Medical Procedures in the Pathogenesis of Cancer and Ischemic Heart Disease: Dose-Response Studies with Physicians per 100,000 Population. San Francisco , CA : CNR Books; 1999.
92. Gofman J W. Preventing Breast Cancer: The Story of a Major, Proven, Preventable Cause of This Disease . 2nd ed. San Francisco , CA : CNR Books; 1996.
93. Sarno JE. Healing Back Pain: The Mind-Body Connection . Warner Books; 1991.
94. Siu AL, Sonnenberg FA, Manning WG, et al. Inappropriate use of hospitals in a randomized trial of health insurance plans. N Engl J Med . 1986 Nov 13;315(20):1259-66.
95. Siu AL, Manning WG, Benjamin B. Patient, provider and hospital characteristics associated with inappropriate hospitalization. Am J Public Health . 1990 Oct;80(10):1253-6.
96. Eriksen BO, Kristiansen IS, Nord E, et al. The cost of inappropriate admissions: a study of health benefits and resource utilization in a department of internal medicine. J Intern Med . 1999 Oct;246(4):379-87.
97. Showalter E. Hystories: Hysterical Epidemics and Modern Media . New York , NY : Columbia University Press; 1997.
98. Fugh-Berman A. Alternative healing. In: Smith B, Steinem G, Mink G, Navarro M, and Mankiller W, eds. The Reader’s Companion to U.S. Women’s History. New York , NY : Houghton Mifflin; 1998. Available at: http://college.hmco.com/history/readerscomp/women/html/wh_001200_alternativeh.htm .
99. Thacker SB, Stroup D, Chang M. Continuous electronic heart rate monitoring for fetal assessment during labor (Cochrane Review). In: The Cochrane Library, issue 1, 2003. Oxford : Update Software.
100. Cole C. Admission electronic fetal monitoring does not improve neonatal outcomes . J Fam Pract . 2003 Jun;52(6):443-4.
101. Nelson HD, Humphrey LI, Nygren P, Teutsch SM, Allan JD. Postmenopausal hormone replacement therapy: scientific review. JAMA . 2002 Aug 21;288(7):872–81.
102. Nelson HD. Assessing benefits and harms of hormone replacement therapy: clinical applications. JAMA . 2002 Aug 21;288(7):882-4
103. Fletcher SW, Colditz GA. Failure of estrogen plus progestin therapy for prevention. JAMA . 2002 Jul 17;288(3):366-8.
104. Rossouw JE, Anderson GL, Prentice RL, et al; Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA . 2002 Jul 17;288(3):321-33.
105. Rutkow IM. Obstetric and gynecologic operations in the United States , 1979 to 1984. Obstet Gynecol . 1986 Jun;67(6):755-9.
106. Family Practice News . February 15, 1995 : 29.
107. Sakala C. Medically unnecessary cesarean section births: introduction to a symposium. Soc Sci Med . 1993 Nov;37(10):1177-98.
108. VanHam MA, van Dongen PW, Mulder J. Maternal consequences of cesarean section. A retrospective study of intra-operative and postoperative maternal complications of cesarean section during a 10-year period. Eur J Obstet Reprod Biol . 1997 Jul;74(1):1-6.
109. Weiner J. Smoking and cancer: the cigarette papers: how the industry is trying to smoke us all . The Nation . January 1, 1996 :11-18.
110. Tobacco.org. Tobacco timeline. Available at: http://www.tobacco.org/resources/history/tobacco_history.html. Acccessed December 16, 2003 .
111. Lasser KE, Allen PD, Woolhandler SJ, Himmelstein DU, Wolfe SM, Bor DH. 2002. Timing of new black box warnings and withdrawals for prescription medications. JAMA . 2002 May 1;287(17):2215-20.
112. Injuryboard.com. General Accounting Office study sheds light on nursing home abuse. July 17, 2003 . Available at: http://www.injuryboard.com/view.cfm/Article=3005. Accessed December 17, 2003 .
113. Weingart SN, McL Wilson R, Gibberd RW, Harrison B. Epidemiology of medical error. West J Med . 2000 Jun;172(6):390-3.
114. Blendon R, Schoen C, et al. Five nation survey exposes flaws in the U.S. health care system. Health Affairs . May/June 2002.
115. Institute of Medicine . Care Without Coverage: Too Little, Too Late . May 21, 2002 . A Shared Destiny: Community Effects of Uninsurance . March 6, 2003 .
116. US Department of Health and Human Services and US Department of Justice. Health Care Fraud and Abuse Control Program Annual Report for FY 1998. April 1999. Health Care Fraud and Abuse Control Program Annual Report for FY 2001. April 2002.
117. Abuse of residents is a major problem in U.S. nursing homes [transcript]. CNN television. July 30, 2001 117 a. Available at: http://www.house.gov/waxman. Accessed December 17, 2003 .
118. Mitka M. Unacceptable nursing home deaths unautopsied. JAMA . 1998 Sep 23-30;280(12):1038-9
119. New data is in on North Carolina ‘s nursing home residents. Medical Review of North Carolina, Inc. July 21, 2003 .
120. Weinstein RA. Nosocomial infection update. Emerg Infect Dis . 1998 Jul-Sep;4(3):416-20.
121. Centers for Medicare & Medicaid Services. Report to Congress: Appropriateness of Minimum Nurse Staffing Ratios In Nursing Homes: Phase II Final Report . December 24, 2001 .
122. Consumer group criticizes Thompson letter dismissing report on dangerous staffing levels in nursing homes [news release]. Washington , DC : National Citizens’ Coalition for Nursing Home Reform. March 22, 2002 .
123. Bergstrom N, Braden B, Kemp M, Champagne M, Ruby E. Multi-site study of incidence of pressure ulcers and the relationship between risk level, demographic characteristics, diagnoses and prescription of preventive interventions . J Am Geriatr Soc . 1996 Jan;44(1):22-30.
124. Miles SH. Concealing accidental nursing home deaths. HEC Forum . 2002 Sep;14(3):224-34.
125. Corey TS, Weakley-Jones B, Nichols GR 2nd, Theuer HH. Unnatural deaths in nursing home patients. J Forensic Sci . 1992 Jan;37(1):222-7.
126. Lloyd-Jones DM, Martin DO, Larson MG, Levy D. Accuracy of death certificates for coding coronary heart disease as the cause of death. Ann Intern Med . 1998 Dec 15;129(12):1020-6.
127. Thomas DR , Zdrowski CD, Wilson MM, et al. Malnutrition in subacute care. Am J Clin Nutr . 2002 Feb;75(2):308-13.
128. Robinson BE. Death by destruction of will. Lest we forget. Arch Intern Med . 1995 Nov 13;155(20):2250-1.
129. Capezuti E, Strumpf NE, Evans LK, Grisso JA, Maislin G. The relationship between physical restraint removal and falls and injuries among nursing home residents . J Gerontol A Biol Sci Med Sci . 1998 Jan;53(1):M47-52.
130. Phillips CD, Hawes C, Fries BE. Reducing the use of physical restraints in nursing homes: will it increase costs? Am J Public Health . 1993 Mar;83(3):342-8.
131. Miles SH, Irvine P. Deaths caused by physical restraints. Gerontologist . 1992 Dec;32(6):762-6.
132. Annas GJ. The last resort—the use of physical restraints in medical emergencies. N Engl J Med . 1999 Oct 28;341(18):1408-12.
133. Parker K, Miles SH. Deaths caused by bedrails. J Am Geriatr Soc . 1997 Jul;45(7):797-802.
134. Miles SH. Concealing accidental nursing home deaths. HEC Forum . 2002 Sep;14(3):224-34.
135. Katz PR, Seidel G. Nursing home autopsies. Survey of physician attitudes and practice patterns. Arch Pathol Lab Med . 1990 Feb;114(2):145-7.
136. Overmedication of U.S. seniors. Reuters Health. May 21, 2003 .
137. Average number of prescriptions by HMOs increases. Drug Benefit Trends . 2002 Sep 12;14(8).
138. Kaiser Family Foundation. Prescription Drug Trends . November 2001.
139. Williams BR, Nichol MB, Lowe B, Yoon PS, McCombs JS, Margolies J. Medication use in residential care facilities for the elderly. Ann Pharmacother . 1999 Feb;33(2):149-55.
140. AARP. Medicare and prescription drugs. Available at: http://www.aarp.org/prescriptiondrugs. Accessed December 16, 2003 .
141. California reaches $100 million multi-state settlement with drug giant Mylan over alleged price-fixing scheme [press release]. Sacramento , CA : Office of the Attorney General, Department of Justice, State of California ; July 12, 2000 .
142. Attorney general reaches settlement with drug giant. WRAL News. March 7, 2003 . Available at: . http://www.wral.com/money/2026364/detail.html . Accessed December 16, 2003 .
143. Blowing the final whistle. The Observer. November 25, 2001 . Available at: http://education.guardian.co.uk/businessofresearch/comment/0,9976,606260,00.html. Accessed December 16, 2003 .
144. AARP. Are food supplements for me. Available at: http://www.aarp.org/Articles/a2003-03-07-supplements.html. Accessed December 16,2003 .
145. Bernabei R, Gambassi G, Lapane K, et al. Management of pain in elderly patients with cancer. SAGE study group. Systematic assessment of geriatric drug use via epidemiology. JAMA . 1998 Jun 17;279(23):1877-82.
146. Associated Press. Panel names estrogen as carcinogen. The Washington Post . December 16, 2000 :A05.
147. Estrogen hikes ovarian cancer risk. MSNBC staff and wire reports. July 16, 2002 . Grady D. Study recommends NOT using hormone therapy for bone loss. New York Times . October 1, 2003 .
148. Anderson GL, Judd HL, Kaunitz AM, et al. Effects of estrogen plus progestin on gynecologic cancers and associated diagnostic procedures: the Women’s Health Initiative randomized trial. JAMA . 2003 Oct 1;290(13):1739-48.
149. Chlebowski RT, Hendrix SL, Langer RD , et al. Influence of estrogen plus progestin on breast cancer and mammography in healthy postmenopausal women: the Women’s Health Initiative randomized trial. JAMA . 2003 Jun 25;289(24):3243-53.
150. Wassertheil-Smoller S, Hendrix SL, Limacher M, et al . Effect of estrogen plus progestin on stroke in postmenopausal women: the Women’s Health Initiative: a randomized trial. JAMA . 2003 May 28;289(20):2673-84.
151. Shumaker SA, Legault C, Rapp SR, et al. Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in postmenopausal women: the Women’s Health Initiative memory study: a randomized controlled trial. JAMA 2003;289:2651-62 .
152. Beral V; Million Women Study Collaborators. Breast cancer and hormone-replacement therapy in the Million Women Study. Lancet . 2003 Aug 9;362(9382):419-27.
••••
This article (Doctors Kill 1,000,000 People Each Year In the U.S. Alone Shocking Health Statistics) was originally created and published by RELFE and is republished here with permission and attribution to publisher Stephanie Relfe and relfe.com.Copyright ©Stephanie Relfe 2015 -3000••••

••••
Stay tuned to …

••••
The Liberty Beacon Project is now expanding at a near exponential rate, and for this we are grateful and excited! But we must also be practical. For 7 years we have not asked for any donations, and have built this project with our own funds as we grew. We are now experiencing ever increasing growing pains due to the large number of websites and projects we represent. So we have just installed donation buttons on our websites and ask that you consider this when you visit them. Nothing is too small. We thank you for all your support and your considerations … (TLB)••••
Comment Policy: As a privately owned web site, we reserve the right to remove comments that contain spam, advertising, vulgarity, threats of violence, racism, or personal/abusive attacks on other users. This also applies to trolling, the use of more than one alias, or just intentional mischief. Enforcement of this policy is at the discretion of this websites administrators. Repeat offenders may be blocked or permanently banned without prior warning.••••
Disclaimer: TLB websites contain copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available to our readers under the provisions of “fair use” in an effort to advance a better understanding of political, health, economic and social issues. The material on this site is distributed without profit to those who have expressed a prior interest in receiving it for research and educational purposes. If you wish to use copyrighted material for purposes other than “fair use” you must request permission from the copyright owner.••••
Disclaimer: The information and opinions shared are for informational purposes only including, but not limited to, text, graphics, images and other material are not intended as medical advice or instruction. Nothing mentioned is intended to be a substitute for professional medical advice, diagnosis or treatment.
Dead Newborn Infant Lies In Gutter Like Trash In ChinaSource: Marie Claire magazine, June 2001A morning in the Chinese province of Hunan brings an unimaginable sight of cruelty and horror. Lying in the gutter of a bustling main road is the tiny, twisted body of a dead baby girl. She is naked, surrounded by only dirty pieces of hospital gauze. Buses and bicycles speed past the corpse, spraying it with mud.Nameless and unwanted, the newborn’s been dumped by the roadside during winter. Few of the locals hurrying by give her a second glance. To them, she is just one of thousands of baby girls abandoned each year as a result of China’s ruthless one-child policy. “I think the baby had just died,” says a woman who was the only person to attempt to rescue the infant. “I touched her skin, and it was warm. Blood was still coming out of her nose.”Under China’s strict family-planning laws, couples in urban areas are allowed only one child; couples in most rural regions can try for a second if their first-born is a girl. Those who have an illegal baby are subject to crippling fines, sterilization, and other severe penalties. To avoid punishment, many parents go to the desperate measure of deserting their illegal offspring. If their child is a girl--considered less valuable than boys in rural, traditional parts of China, like Hunan--the chances of this heartbreaking fate are immeasurably higher.To the Chinese authorities, abandoned girls are merely worthless trash. “I called the emergency services, but nobody came,” says the woman who found this latest little victim. (For fear of official reprisal, she wishes to remain anonymous.) “The baby was lying right near the government tax office, so many people in government just walked past.” Eventually, an old man picked up the child, put her in a box, and dropped her in a garbage bin. When the police finally arrived, they showed no interest in investigating her death. They instead arrested the woman who’d tried to save her. “I took some photographs, because it was so terrible; the police were more worried about my pictures than the baby,” she says. The police only released the woman once she handed over her film.The chilling death of this baby, and countless others like her, reveals the gross inhumanity behind the enforcement of China’s one-child policy. The world’s most populous country with 1.3 billion people, China introduced the policy in 1979 in response to a rapid increase in the birth rate under former leader Mao Tse-tung, and a fear that the exploding population couldn’t be fed. Today, China’s leaders claim that the policy has been a great success, preventing an extra 300 million births.Most Chinese recognize the need to keep the birth rate down, but the government’s methods continue to cause untold misery. “What’s happening since the one-child policy was introduced as a national catastrophe,” says Wu Hongli a woman’s aid worker in Shanghai who does outreach work in rural communities. “So many families have lost their children and had their lives destroyed.”While abandonment is shockingly common, say Wu, some parents who give birth “outside the plan” are so terrified of being caught, they even kill their child. “One father dropped his daughter down an old well so no one would ever know she existed.”Each region in China has a target “birth quota” for the number of babies allowed to be born per year. Local government offices and state-owned factories appoint female staff to monitor every woman’s menstrual cycle. Before conceiving a baby, women must have a “birth permit”; those who don’t, or who’ve already given birth have their contraceptive usage monitored. Though condoms and the Pill are available, the most common form of birth control is the metal IUD; it’s inserted at government clinics and detectable by X-ray to ensure it hasn’t been removed without authorization.Click to enlarge
Officially, the state condemns the use of force or cruelty in enforcing quotas. But in practice, officials feel pressure to achieve low birth rates or face disgrace and demotion, causing many to resort to brutal tactics. Population officials, “abortion squads” regularly conduct midnight raids into the homes of women suspected of becoming pregnant illegally. These squads drag offenders into custody and detain them until they submit to an abortion, even if they’re eight to nine months pregnant.Gao Xio Duan, a former population-control official who fled to America three years ago, spoke out about the methods used to terminate illegal pregnancies. Describing herself as a “monster”, she told a U.S. Congressional committee how she had helped doctors inject lethal formaldehyde into babies’ skulls during forced abortions. “I saw how the baby’s lips were sucking and how its limbs were stretching,” she said of one such instance. “Then the doctor injected the poison into its head, and the child died and was thrown in the trash.”Some pregnant women try to avoid capture by going into hiding. But often, they return after the birth to find their homes burned to the ground and their other family members beaten or persecuted. In an extreme case last year, a man in Changsha, a Hunan province, died after being tortured for refusing to reveal the whereabouts of his pregnant wife. If couple successfully give birth to an illegal baby, the face further punishment, including fines of around 10,000 yuan ($1500)--seven times more than the average peasant’s annual income--compulsory sterilization, forced confiscations of property. Children born this way are denied schooling, medical care, and other social benefits.Many peasants believe only sons can carry on the family line. “They think it greatly dishonors their ancestors if they don’t produce a male heir,” says outreach worker Wu Hongli. Also, daughters usually live with their husband’s family after marriage and are, therefore, considered a wasted investment. “Although the one-child policy allows many rural couples to have another baby if their first is a girl, it spells disaster if their second child is also female,” says Wu. Such unwanted girls are often dubbed “maggots in the rice”. In northeast China, one man was so distraught when his second-born was a girl that he smothered bother her and his other healthy daughter. “It is a sin not to have a boy. I will try again for a son when I get out of prison,” he told police.In China’s modern cities, the traditional desire for boys has all but disappeared. But coupled with the one-child policy, its endurance in the country side is having devastating social consequences. An estimated 17 million girls are “missing” from the population nationwide. Infanticide and abandonment account for some of these lost females, with those who survive ending up in bleak state orphanages--if they’re lucky. Other factors include sex-selective abortion, which are technically outlawed, but are still readily available through the use of ultrasound for a small bribe. According to official figures, 97.5 percent of all aborted fetuses in China are female. Failure to register the birth of girl babies is another factor; it’s believed many parents hide their daughters, or sell them to infertile couples, thereby making them invisible to authorities.The result is a chronic imbalance in the male and female populations. Already, millions of rural Chinese men are unable to find a wife. To overcome this, young girls who leave their villages to look for work are often tricked and drugged by traffickers and then sold to older single men in distant provinces, where they don’t even speak the same dialect. This imbalance is set to worsen, too. A decade ago, the birth records of boys versus girls in some countryside areas where two to one. Today, the ratio is often as high as an alarming six to one.Still, the Chinese government remains committed to its one-child policy. Wu Hongli despairs over this situation. “Of course, population is a serious issue,” she says, “but so are human rights. The authorities are making no attempt to implement more humane family planning.” She also laments official apathy toward teaching the population about the equal value of baby girls. “Educational programs have had a lot of success in rural areas, but there is still a vast amount to be done. So many tragedies are ignored every day that it makes me want to cry. ”Looking at the anonymous baby girl whose brief life ended on a roadside only a few weeks ago, it’s impossible not to feel the same way.
SCOOP – Toute honte bue, le gouvernement fait un virage à 180° et donne raison (sans le dire publiquement) au professeur Raoult : il généralise le recours à l’hydoxychloroquine et même sa vente au public !
Enfin la raison l’emporte après, hélas, un temps précieux – au moins un mois – perdu par nos politiques amateurs, voire criminels, à ne savoir quoi faire et à se dédire, alors que des scientifiques de renom – le Professeur Didier Raoult et ses collaborateurs de l’IHU de Marseille – montraient la voie à emprunter. La volte-face est telle que l’hydroxychloroquine peut même être prescrite en ambulatoire sous contrôle médical. On ne peut que se féliciter d’une telle décision arrachée de haute lutte par la pression populaire – une pétition ayant récolté plus de 200 000 signatures en très peu de temps -, mais il restera malgré tout à exiger des comptes aux pieds nickelés qui nous gouvernent, une fois vaincue cette calamité.

Le scandale devenait trop énorme.
La colère émanant des dizaines de milliers de patients devenait trop ingérable.
L’accumulation des témoignages de personnes guéries par la prescription du Professeur Raoult devenait trop embarrassante.
La comparaison avec les décisions prises à l’étranger – où tous les pays du monde se ruent sur l’hydroxychloroquine – devenait trop injustifiable.
Le risque de voir les ministres traduits devant la Cour de Justice de la République devenait trop certain (une pétition en ce sens vient déjà de dépasser les 200.000 signatures !)
Bref, Macron et Philippe viennent de céder. Malgré la pression criminelle des lobbys pharmaceutiques, furieux de voir un pactole leur échapper car la chloroquine ne coûte et ne rapporte presque rien, les pieds nickelés qui croient nous gouverner viennent de faire un virage à 180°.
De façon minable, en catimini, toute honte bue.
Le Journal Officiel de ce 26 mars 2020 acte un virage à 180° sur l’hydoxychloroquine
Le Journal Officiel de la République française (JORF n°0074) de ce jeudi 26 mars 2020 vient de publier, en fin de matinée, un “décret n° 2020-314 du 25 mars 2020” présenté comme “complétant le décret n° 2020-293 du 23 mars 2020 prescrivant les mesures générales nécessaires pour faire face à l’épidémie de covid-19 dans le cadre de l’état d’urgence sanitaire”.
Qu’y découvre-t-on ? Ceci :
« Chapitre 7« Dispositions relatives à la mise à disposition de médicaments
« Art. 12-2. – Par dérogation à l’article L. 5121-8 du code de la santé publique, l’hydroxychloroquine et l’association lopinavir/ritonavir peuvent être prescrits, dispensés et administrés sous la responsabilité d’un médecin aux patients atteints par le covid-19, dans les établissements de santé qui les prennent en charge, ainsi que, pour la poursuite de leur traitement si leur état le permet et sur autorisation du prescripteur initial, à domicile.
« Les médicaments mentionnés au premier alinéa sont fournis, achetés, utilisés et pris en charge par les établissements de santé conformément à l’article L. 5123-2 du code de la santé publique.
« Ils sont vendus au public et au détail par les pharmacies à usage intérieur autorisées et pris en charge conformément aux dispositions du deuxième alinéa de l’article L. 162-17 du code de la sécurité sociale. Le cas échéant, ces dispensations donnent lieu à remboursement ou prise en charge dans ce cadre sans participation de l’assuré en application des dispositions de l’article R. 160-8 du même code. L’Agence nationale de sécurité du médicament et des produits de santé est chargée, pour ces médicaments, d’élaborer un protocole d’utilisation thérapeutique à l’attention des professionnels de santé et d’établir les modalités d’une information adaptée à l’attention des patients.
« Le recueil d’informations concernant les effets indésirables et leur transmission au centre régional de pharmacovigilance territorialement compétent sont assurés par le professionnel de santé prenant en charge le patient dans le cadre des dispositions réglementaires en vigueur pour les médicaments bénéficiant d’une autorisation de mise sur le marché.
« La spécialité pharmaceutique PLAQUENIL© et les préparations à base d’hydroxychloroquine ne peuvent être dispensées par les pharmacies d’officine que dans le cadre d’une prescription initiale émanant exclusivement de spécialistes en rhumatologie, médecine interne, dermatologie, néphrologie, neurologie ou pédiatrie ou dans le cadre d’un renouvellement de prescription émanant de tout médecin.
« Afin de garantir l’approvisionnement approprié et continu des patients sur le territoire national, en officines de ville comme dans les pharmacies à usage intérieur, l’exportation des spécialités contenant l’association lopinavir/ritonavir ou de l’hydroxychloroquine est interdite. Ces dispositions ne s’appliquent pas à l’approvisionnement des collectivités relevant des articles 73 et 74 de la Constitution et de la Nouvelle-Calédonie.
« Pour l’application du présent article, sont considérés comme établissements de santé les hôpitaux des armées, l’Institution nationale des Invalides et les structures médicales opérationnelles relevant du ministre de la défense déployées dans le cadre de l’état d’urgence sanitaire. ».
Sources :
cf. photo jointe ci-dessus
et source directe sur le site du Journal Officiel ici
CONCLUSION : un gouvernement irresponsable et criminel qui aurait dû prendre ces mesures il y a un mois
On notera ainsi que le gouvernement fait un virage à 180° et donne totalement raison aux demandes du Professeur Raoult, qui réclamait ces décisions depuis un mois :
1) – la vente et la prescription d’hydroxychloroquine est désormais possible partout, y compris la vente au public sur prescription médiale ;
2)- pour tenter de “sauver la face” et pour satisfaire les lobbyistes cupides de “Big Pharma”, le même décret parle des antirétroviraux lopinavir/ritonavir qui rapportent, eux, beaucoup d’argent aux grands laboratoires pharmaceutiques.
Mais une étude venue de Chine et rendue publique le 24 mars vient de montrer que ces médicaments destinés à lutter contre le VIH (SIDA) ne donnent aucun résultat et, pire, produisent même des “événements indésirables digestifs plus fréquents” que dans le groupe avec placebo.
Source : https://www.lequotidiendumedecin.fr/specialites/infectiologie/un-premier-essai-decevant-pour-le-lopinavir-ritonavir
3)- la France interdit discrètement “l’exportation des spécialités contenant l’association de l’hydroxychloroquine”.
—————
En bref, la défaite intellectuelle, politique, scientifique, sanitaire et morale de Macron et de son gouvernement est totale et absolue. Il n’en est que plus justifié encore de saisir la Cour de Justice de la République.
François Asselineau
26 mars 2020 – 13h00
UPR [Union Populaire Républicaine]
Nous en avons déjà parlé à plusieurs reprises, la vitamine C à hautes doses peut être très efficace comme l’avait démontré en son temps, le professeur et double prix Nobel Linus Pauling. Mais attention, il s’agit de prendre 10 g de vitamine C par jour et non quelques centaines de milligrammes. Vous pourrez trouver un grand nombre d’informations ainsi que le moyen de fabriquer de la vitamine C liposomale dans la brochure Vitamine C liposomale et cancer. Dans cet hôpital new-yorkais il s’agit d’injecter en intraveineuse jusqu’à 6 g par jour en 3 à 4 fois ; la vitamine C est immédiatement disponible dans l’organisme. Lorsqu’il s’agit de l’avaler et de passer par voie intestinale, il y aura toujours une perte, c’est pourquoi il faut prendre une dose un peu plus grande, de 10 grammes environ. Cela se fera dans un grand verre d’eau, après avoir mangé afin d’éviter quelques gargouillis désagréables. Tout excès de vitamine C finira par être éliminé par les urines.

Des patients atteints de coronavirus gravement malades dans le plus grand système hospitalier de l’État de New York reçoivent des doses massives de vitamine C – selon des rapports prometteurs selon lesquels cela a aidé les gens dans une Chine durement touchée, a appris The Post.
Le Dr Andrew G. Weber, pneumologue et spécialiste des soins intensifs affilié à deux établissements de santé Northwell à Long Island, a déclaré que ses patients en soins intensifs atteints du coronavirus reçoivent immédiatement 1 500 milligrammes de vitamine C. par voie intraveineuse.
Des quantités identiques du puissant antioxydant sont ensuite réadministrées trois ou quatre fois par jour, a-t-il déclaré.
Chaque dose représente plus de 16 fois l’apport nutritionnel quotidien recommandé en vitamine C du National Institutes of Health, qui n’est que de 90 milligrammes pour les hommes adultes et de 75 milligrammes pour les femmes adultes.
Le régime est basé sur des traitements expérimentaux administrés à des personnes atteintes du coronavirus à Shanghai, en Chine, a déclaré Weber.
« Cela aide énormément, mais ce n’est pas mis en évidence parce que ce n’est pas une drogue sexy. »
Un porte-parole de Northwell – qui exploite 23 hôpitaux, dont l’hôpital Lenox Hill dans l’Upper East Side de Manhattan – a déclaré que la vitamine C était « largement utilisée » comme traitement contre les coronavirus dans tout le système, mais a noté que les protocoles de médication variaient d’un patient à l’autre.
« Comme le clinicien le décide », a déclaré le porte-parole Jason Molinet.
Environ 700 patients sont traités pour le coronavirus à travers le réseau hospitalier, a déclaré Molinet, mais on ne sait pas combien reçoivent le traitement à la vitamine C.
Mardi, les hôpitaux de New York ont la permission fédérale de donner un cocktail d’hydroxychloroquine et d’azithromycine à des patients désespérément malades sur la base de « soins de compassion ». La vitamine C est administrée en plus de médicaments tels que l’hydroxychloroquine, un antipaludéen, l’antibiotique azithromycine, divers produits biologiques et des anticoagulants, a déclaré Weber.
Le président Trump a tweeté que la thérapie combinée non éprouvée a « une réelle chance d’être l’un des plus grands changeurs de jeu de l’histoire de la médecine ».
Weber, 34 ans, a déclaré que les niveaux de vitamine C chez les patients atteints de coronavirus diminuent considérablement lorsqu’ils souffrent de septicémie, une réponse inflammatoire qui se produit lorsque leur corps réagit de manière excessive à l’infection.
« Il est tout à fait logique dans le monde d’essayer de maintenir ce niveau de vitamine C », a-t-il déclaré.
Un essai clinique sur l’efficacité de la vitamine C par voie intraveineuse chez les patients atteints de coronavirus a débuté le 14 février à l’hôpital Zhongnan de Wuhan, en Chine, l’épicentre de la pandémie.
L’étude randomisée en triple aveugle impliquera environ 140 participants et devrait être terminée d’ici le 30 septembre, selon les informations publiées sur le site Web de la US National Library of Medicine.
Photo d’illustration : comprimés de vitamine C – Getty Images / iStockphoto
24 mars 2020
Concernant cette épidémie de Coronavirus, l’intervention de l’ancien directeur au CNRS à la réputation internationale rejoint l’avis de beaucoup d’entre nous qui pensent que lorsque l’on n’a rien à proposer, que l’on manque de lits d’hôpitaux, de masques, de gel hydroalcoolique et de plein d’autres matériels de protection, il est suicidaire et criminel de se passer d’un tel traitement ! C’est aussi simple que ça.
Ancien directeur de recherche au CNRS, mondialement connu pour ses travaux sur les virus géants, Jean-Michel Claverie réagit à la polémique sur la chloroquine, que le professeur Didier Raoult promeut comme traitement contre le coronavirus.
« Pourquoi ne pas essayer l’hydroxychloroquine in vivo ? », autrement dit, cet anti-paludéen recommandé par le Pr Didier Raoult sur les personnes contaminées par le coronavirus, interroge Jean-Michel Claverie, professeur émérite de génomique et bioinformatique à l’école de médecine d’Aix-marseille. L’administrer, c’est peu ou prou pratiquer « de la médecine de guerre », comme il l’a déclaré à Sciences et Avenir. Et ce, lors d’une crise sanitaire due au coronavirus Sars-CoV-2 comme celle que nous sommes en train de vivre. Lors d’une atteinte de Covid-19, « c’est bien sûr le plus tôt possible qu’il faut administrer (cette hydroxychloroquine) pour enrayer l’évolution vers la pneumonie ». C »est ainsi qu’il s’exprime dans la « Revue politique et parlementaire », dans un article intitulé « Plaquenil : trop tard ne vaut pas mieux que jamais« . L’ancien directeur de recherche au CNRS, mondialement connu pour ses travaux sur les virus géants, récompensé en novembre 2019 avec Chantal Abergel par le prix Jaffé de l’ Académie des sciences, y dénonce comme une « absurdité des demi-mesures politiques guidées par la volonté de ne déplaire ni aux uns (le corps médical), ni aux autres (le grand public) (…) la décision récente qui restreint l’utilisation du Plaquenil aux malades en « état grave » (c’est-à- dire en pleine pneumonie) ». Rappelons que le Plaquenil est le nom commercial de l’hydroxychloroquine. Il a accepté de répondre aux questions de Sciences et Avenir.
Sciences et Avenir : Un essai clinique européen vient d’être décidé, où sera évaluée l’efficacité de l’hydroxychloroquine. Pourquoi y voyez-vous une absurdité ?
Jean-Michel Claverie : Ce qui me scandalise, c’est que d’ici aux résultats du test, on aura des milliers de morts. Mieux vaut de faux espoirs que de vrais morts. On sait que l’hydroxychoroquine est efficace in vitro pour détruire le virus, pourquoi ne pas l’essayer sur les malades du Covid-19 ? Et le plus tôt possible, sans attendre que la maladie soit à un stade sévère où les poumons sont déjà fortement atteints. On se dit, comme dans la médecine de guerre, on va essayer ça ! Quand les poumons sont trop abîmés, détruire le virus à ce stade est inutile.
Ce n’est pas très scientifique…
Depuis quand la médecine, c’est scientifique ? J’ai enseigné à mes étudiants le concept d' »evidence-based medicine » (la médecine basée sur les preuves). Mais j’ai été étonné de découvrir à quel point ce paradigme était récent ! Il date des années 1970 : peut-être 90% des traitements n’ont pas été élaborés de cette manière et on ne connaît pas le mode d’action cellulaire précis de la plupart des médicaments.
Aux premières annonces du Pr Raoult, beaucoup de critiques ont dit : » À chaque fois qu’un virus apparaît, on nous ressort la chloroquine », laissant ainsi entendre que ce n’était peut-être pas sérieux…
À la vitesse où se développe la maladie, on pourrait être fixé dans les quinze jours qui viennent. En attendant, il faut essayer. La chloroquine agit en bloquant dans les cellules une étape d’acidification nécessaire pour que le virus (un virus à ARN) démarre sa multiplication. Certaines membranes ne pouvant se fusionner, il demeure en quelque sorte bloqué dans la porte d’entrée de la cellule. C’est ce que l’on constate au laboratoire et si cela se passe aussi chez les malades du Covid-19, alors ce serait effectivement la première fois que ce blocage bien démontré » in vitro » se traduira par une efficacité sur les malades, » in vivo « .
Il y a eu une étude chinoise, que cite le Pr Raoult comme inspirante ?
Oui, publiée dans Cell Research, une revue scientifique de bon niveau international. Une étude où étaient donnés les résultats obtenus contre le coronavirus avec 4 drogues, dont le remdesivir, un antiviral qui va aussi être testé, à l’instar de la chloroquine, dans l’essai européen dont nous parlions ci-dessus. Ce dont il faut se souvenir, c’est que les médecins, dans les moments de crise, n’ont pas attendu que tout soit vérifié scientifiquement pour agir. Inutile de rappeler comment Pasteur lui-même a » inventé » et testé son vaccin contre la rage…
L’étude menée par le Pr Raoult, sur seulement 24 patients, est fortement critiquée !
Si ce qui est écrit dans cette étude reproduit ce qui s’est vraiment passé avec les patients (20 ne présenteraient plus de charge virale après 6 jours), je considère que cette étude est statistiquement significative.
Et donc, vous prescririez de l’hydroxychloroquine.
Si j’étais médecin, ça ne m’ennuierait pas. Il y des dizaines de millions de personnes qui en ont absorbé, moi-même j’en ai beaucoup mangé pendant les dix ans où j’ai vécu en Afrique. Les effets secondaires sont bien moindres que l’effet du médicament qui interfère avec le parasite du paludisme par le même effet d’acidification cellulaire dont nous avons parlé.
Comment a été reçu votre article de la « Revue politique et parlementaire », tout juste paru ?
Après partage sur la liste du collectif Inter-hopitaux animée par le Prof. André Grimaldi qui compte près de 500 hospitalo-universitaires de toute la France, je n’ai eu aucun retour négatif et plusieurs ont abondé dans mon sens, y compris un célèbre découvreur d’un non moins célèbre virus. J’y expose que la Science ne doit pas devenir la justification de la perte généralisée du goût du risque de notre société, et qu’il faut garder aux médecins la possibilité d’essayer des traitements non-encore étayés par des études statistiques indiscutables, tant qu’ils sont basés sur des hypothèses raisonnables, et sans danger important pour leurs patients. Le principe de précaution ne doit pas inhiber toute velléité d’innovation.
Photo d’illustration : Médicament : une boîte de Plaquenil. CRÉDIT MATHIEU PATTIER/ SIPA
Dominique Leglu
Sciences et Avenir
25 mars 2020
Jeranism Friday Lounge #18 - What's Next? - March 13, 2020
tps://www.youtube.com/watch?v=mV3VGrJZI70&t=725s
149K subscribersAnother Friday Lounge Show where we ask the question... What's Next? Please subscribe to those panel members you enjoy below! All show links will be listed below following the live stream. Enjoy the show!
Rodrigo Ferrari-Nunes https://www.youtube.com/channel/UCw0-... https://www.patreon.com/anthropology
Iru Landucci https://www.youtube.com/channel/UChPB... https://www.youtube.com/channel/UCZG-... https://www.patreon.com/nurparatodos http://www.nurparatodos.com.ar
Globebusters https://www.youtube.com/channel/UCXIo... http://patreon.com/globebusters
UAP https://www.youtube.com/channel/UCnK3... https://www.youtube.com/channel/UCO3n... Karen B https://www.youtube.com/channel/UChDZ...
COVID-19, HAITI, ISRAEL, HOLLYWOOD, DISNEY, CHILD SEX TRAFFICKING, PORN, SUICIDE-MURDERS, PEDO-CRIMINALS, CLINTONS, OXFAM, TRUDEAU, Q ANON.

GODLESS 2019-2020 COVID-19 TRIED TO MASK ALL THESE ABOMINATIONS...
... HAITI, ISRAEL, HOLLYWOOD, DISNEY, CHILD SEX TRAFFICKING, PORN, SUICIDE-MURDERS, PEDO-CRIMINALS, CLINTONS, OXFAM, TRUDEAU, HOLLYWOOD, DISNEY, ...
YOU CANNOT SCARE MUSLIMS WITH YOUR COVID-19 AND YOU KNOW IT!
FRENCH ZIONIST BERNARD HENRI-LÉVI AND THE TALMUDIST MAFIA, THE MASS MURDERERS OF LIBYA!
The Cabal, Deep State and QAnon E4 - Child Lovers Everywhere
MOST TOP PEDO-CRIMINALS OF THE TALMUDIC MASONIC QABBALAH ARE FREE AND RULING OVER US!
https://www.youtube.com/watch?v=51rabmB_amk
Fall of the Cabal part 1-5 compiled
https://www.youtube.com/watch?v=ZZpIxq7blNY&t=48s
Fall of the Cabal part 6-10 compiled
Iraqi Political Analyst Muhammad Sadeq Al-Hashemi: Coronavirus Is an American, Jewish Plot to Reduce World Population; Rothschilds Paid for the Annihilation of Native Americans and Scots
https://www.memri.org/tv/iraqi-analyst-sadeq-hashemi-dean-koontz-american-zionist-plot-coronavirus-world-population
https://www.youtube.com/watch?v=idrZ0HnHpSs
#7845 | 02:36
Source: Al-Ayyam TV (Iraq)Iraqi political analyst Muhammad Sadeq Al-Hashemi said in a February 26, 2020 interview on Al-Ayam TV (Iraq) that in the 1981 thriller novel titled The Eyes of Darkness, American author Dean Koontz had written about the coronavirus. Al-Hashemi argued that this proves that coronavirus is an American plot and he said that the goal of the plot is to reduce the world's population. He said that in the past 10 years, two patents have been filed in the United States for the development of virus strains with the name "corona" and he compared this American "conspiracy" to when the Jews used blankets infected with anthrax to wipe out 86% of the native population in what is today the United States in order to have a real Jewish homeland. He said that the Zionist lobby similarly cleansed one third of the population of Scotland and that the Rothschild family has a monopoly of laboratories that develop biological and nuclear weapons. Al-Hashemi added that the Rothschilds had been the ones who decided to use nuclear weapons on Hiroshima and Nagasaki in 1945.Muhammad Sadeq Al-Hashemi: "What proves that [the coronavirus] is American-made and an American plot is that there is a book called Darkness Dwellers [i.e. The Eyes of Darkness] written by Dean Koontz in 1981, 40 years ago. Forty years ago, he already wrote about the coronavirus appearing in Wuhan. He gave [the virus] the same name (?), only adding '400.' The '400' is a riddle I couldn't solve. It's called Corona-400 [in the book]. Before 2015, and also in 2018, two patents were issued in the U.S. to develop a strain of viruses under the same name."Interviewer: "Corona?"Muhammad Sadeq Al-Hashemi: " Yes, corona. The patent is registered in the U.S., with a number and with a date.[...]"The most prominent American economists talk about the need to reduce the world's population."Interviewer: "Right"Muhammad Sadeq Al-Hashemi: "So how can I think well of the U.S., and reject conspiracy theories, when the U.S. is acting in keeping with them? If we study [American] political history, it is based entirely on conspiracies. In order to take root in what is today the United States... America was a British colony, and the Jews planned to cleanse the two Americas, so that they would become the real Jewish homeland, before Israel [was established]. So they spread anthrax through blankets. They annihilated 86% of the population of the U.S. with anthrax. The Zionist lobby used this against the Scottish people, thus killing one third of the population of Scotland. It was also America that put an end to WWII, following a Zionist decision. The decision was taken by the House of Rothschild. The world must speak about the Rothschild family..."Interviewer: "Yes, it is a rich Jewish family..."Muhammad Sadeq Al-Hashemi: "[The Rothschild family] finances and has a monopoly on laboratories that develop biological and nuclear weapons. [The Rothschilds] decided to end [WWII] and financed the attack on Hiroshima and Nagasaki."MARSEILLE
Coronavirus : Actu du 31 Mars 2020 - Efficacité HC Confirmée et fabrication de masques
https://www.youtube.com/watch?v=KUG036zaabc&t=500s
76.3K subscribers

Dean Koontz
“I was a poor kid with a Jewish grandmother and a great-grandmother who was black,” Koontz said. “I grew up in a dirt-poor family. I’m used to the abuse that you take. I don’t dish it out, I never have, and this is just appalling to me. I guess I’ll be smeared with this for the rest of my life. I’m not outraged, I’m not spooked, it’s just -- my sadness is so deep.” Los Angeles Times
The name was GORKI-400 in the 1981 Edition of the book "THE EYES OF DARKNESS" by Dean Koontz. In the 2008 edition the name as changed to WUHAN-400!
1981 Edition ?
2008 Edition where WUHAN-400 replaced GORKI-400
Subscribe to: Post Comments (Atom)The UN Invents Climate Change and COVID-19. What Now?Anthony James Hall from Looking out at the World from CanadaFrom:anthonyjhall@substack.comTo:EVA BRAUN BASHEER AHMADFri, 27 Dec 2024 at 22:47Forwarded this email? Subscribe here for more
The UN Invents Climate Change and COVID-19. What Now?
The gloves are off and the truth is out in the age-old battle for survival.
Dec 27
READ IN APP 

The World Economic Forum (WEF) based in Davos took up the task of acting in 2020 as the PR spin doctor to the pandemic merchants in the health branch of the United Nations. As a result, both the WEF and the UN’s World Health Organization (WHO) have deserved reputations as key promoters of a catastrophic event in world history that continues to kill and maim at least tens of millions of people worldwide.
Looking out at the World from Canada is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
This outcome was not the result of a some sort of horrific mistake. It was rather the outgrowth of a very well-documented and unmistakable plan, developed to reduce the global population as well as diminish the wellbeing and living standards of the survivors.
As shall be demonstrated below, the UN and WEF partners both form key parts of the platform where the depopulation scheme developed along with preparations for the robotic transhumanism of survivors. The ongoing scheme aims to alter dramatically the political economy of the world in order to add to the entitlements of humanity’s most outlandishly privileged minority.
Three weeks before taking Office, Acting US President Donald Trump as well as much of his team decided to withdraw the United States from membership in, and support of, the World Health Organization (WHO).

https://www.ft.com/content/e6061ed5-2703-4b8a-9948-a557aaaf52c2
Trump’s own motivations for leaving the UN’s health department seem not to be based on any genuine reckoning with the horrors of the WHO’s multi-faceted role in providing the cover for the injection attack directed at all branches of humanity.
Trump was the Commander-In-Chief in charge of the US Armed Forces’ preparation of the “Warp Speed” injected bioweapons. As Sasha Latypova and many others have explained it, the jabs were initially developed under the auspices of the Department of Defence. The bioweapons were legally identified as military “countermeasures” in order to evade medical regulations.
The jabs are really gene-altering concoctions disguised as a medical remedy that, we were told, was supposed to stop the spread of a respiratory contagion. Nothing of the sort happened.
There was and is nothing remedial at all in the many billions of clot shots that, according to the COVID score keepers at Johns Hopkins University, have already been injected into the arms of more than half of the world’s population.
For whatever reason Trump remains very far from coming to grips with the scale and utter ruthlessness of the war on humanity initiated by the US Armed Forces. A large body of documentation makes it clear that “all decisions concerning the Covid-19 vaccine research, materials acquisition, distribution, and information sharing were tightly controlled by the Department of Defence.”
https://expose-news.com/2023/01/08/us-dod-controlled-covid-vaccine-from-start/
There has been much informal debate among the well informed concerning how such an unprecedented approach to warfare came about. What possible justification could there be for an injected bioweapon attack on all branches of the human population?
Many believe that those truly behind the assault, with Trump being nothing more than a manipulated figure head, are seeking to reduce, enfeeble, and enslave the human population with the aim of achieving total control over the survivors.
As shall be addressed here, green environmentalism has reached extreme levels of hysteria especially in some closed circles of elitist power. In these closed communities whose members have the wealth and contacts to exercise unbounded influence, average working people are sometimes viewed as cancers uselessly feeding on the deteriorating health of the natural world.
Carbon emissions from all industrial activities that employ and service the masses have been so demonized, that the secret elimination of people for the sake of the environmental rehabilitation is made to seem justifiable.

Trump’s decision to pull the USA out of the WHO is a step in the right direction. The Acting President, however, doesn’t indicate that he fully grasps the implications of what he is about to do. Even with Robert F. Kennedy at his side, Trumps seems blind to the full extent of the onslaught of the lies and crimes in which he remains deeply implicated.
Trump has yet to come to terms with lethal plagues of human devastation enabled by the disinformation given the veneer of legitimacy by well-rewarded shills at the WHO and WEF. Trump continues to delude himself by retaining the illusion that he is the Vaccine Hero of America who saved millions of people who would otherwise have succumbed to the COVID-19 epidemic.
Trump’s decision to remove the USA from the WHO is certainly in line with his promise to Make America Great Again. The decision is certainly in line with preserving and enhancing the apparatus of national sovereignty in order to counter the expansionary agendas of globalist institutions.
Trump’s commitments to put America First, however, are imperilled by his commitment to join with the messianic settlers of Israel in their globalist crusade. The objectives of this ultra-Zionist crusade include the elimination of the Palestinians and the building of the Third Temple on the site of the al Aqsa mosque.
This radical departure is meant to make Jerusalem the imperial capital of a New World Order whose core institution would be a Jewish-dominated World Court. This Court would be a revised Sanhedrin council from the era before the Second Temple was destroyed by Roman Legions in 70 AD.
This globalist vision encompasses the more extreme branches of Israel-First Zionism. This vision is especially well-represented in the anti-Iran war cabinet presently taking shape in the nascent Trump administration. It remains to be seen how recent developments will affect the United Nations with its developing split between different factions.

One faction sees the US-Israeli genocide underway in Gaza and the West Bank as the stuff of major crimes against all of humanity whose perpetrators should face trials and possible punishment to be arbitrated by the judicial branches of the United Nations.
The other faction seeks a continuation of old practices that since 1948 have essentially put Israel and US officials above the law when it comes to the enforcement of international criminal and humanitarian laws. So far Trump has made it very clear he most identifies with those in the second camp who hold devotedly to the conviction that Israel can do no wrong.
Donald Trump’s rejection of the WHO’s globalist incursions into the realm of US sovereignty finds reflection and parallels in many jurisdictions including the Canadian Province of Alberta. In October of 2022 Alberta Premier Danielle Smith declared she was no longer prepared to collaborate with the World Economic Forum under the leadership of Justin Trudeau’s mentor, Klaus Schwab.
Premier Smith made the break in the context of her announcement that she would withdraw from an information-sharing agreement negotiated under the auspices of the WEF. The agreement was between Alberta Health Services and health researchers at Harvard University and at the the Mayo Clinic.
Premier Smith added that, as Alberta’s United Conservative Party’s Leader, “she is in lockstep with federal Conservative Leader Pierre Poilievre, who has stated he and his caucus will having nothing to do with the World Economic Forum.” Premier Smith declared,
"I find it distasteful when billionaires brag about how much control they have over political leaders. That is offensive…the people who should be directing government are the people who vote for them. I think it makes sense to make health decisions based on health experts. As for the group [WEF] and the person at the helm of it [Klaus Schwab] — I don't think he's a medical doctor. I don't think he's a nurse, and I don't think he's a paramedic and I don't think he's a health professional. I am going to be taking advice from our front-line nurses, doctors, paramedics and health professionals to fix the local problems that we have."
https://www.cbc.ca/news/canada/calgary/ucp-world-economic-forum-smith-edmonton-calgary-1.6628294
I have addressed in previous essays how Premier Danielle Smith handled one facet of these discussions with health professionals after she berated the WEF. Dr. William Makis is by far the most outspoken and most high-profile member of this professional class that Premier Smith promised to consult.
As Dr. Makis tells it, he may become the first medical doctor to be jailed in North America for his efforts to explain for Premier Smith, for all Albertans, and for his global audience of Substack subscribers, the systemic and deep-rooted forms of corruption he sees in Alberta Health Service.
PremierDanielle Smith and Dr. William Makis
It is one thing to make a symbolic break with a powerful organization like the WEF. It is quite another thing to leave behind the powerful cultural, commercial and political centres of gravity that such an organization represent. Certainly the Alberta Health Services as presently constituted is a professional proxy of the WEF and of the WHO and of the criminal propensities of the powerful interests directing the actions of both institutions.
This same pattern applies to Donald Trump and his renewed hostility towards the World Health Organization. The WEF has long been wedded not only to the WHO but to the many branches of the United Nations. The WEF is a primary agency at the nexus between the various corporate lobbies that have enormous political and economic clout both inside and outside the United Nations.
This essay will look into the basis of that nexus and the role of corporate moguls, financiers, and public intellectuals that depend heavily on the United Nations and the WEF to push their globalist agendas. Much of the focus of what follows describes how agents of the UN, but especially a Canadian operative working for the Rockefeller dynasty, fixed on the the constructs of “sustainable development” and “environmentalism” as major themes in the advancement of globalist objectives. The individual in question is Maurice Strong.
The Ongoing Cover Up of Crimes Against Humanity
Maurice Strong’s focus on the boundless realm of “the environment” gave rise to an emphasis on the invented boogyman of global warming and climate change. In creating the supposed means to stop this supposed boogyman said to be responsible for expelling so much supposedly toxic CO2 into the atmosphere, Maurice Strong happened on a powerful formula.
Strong realized the effectiveness of manipulating public fears of environmental disaster to impose with minimal resistance social controls targeting especially the then-fairly-prosperous middle class people in the West.
Something of a repeat performance took place when a supposedly “new” coronavirus was publicized by the WHO as a stealthy killer germ. The demonic germ, soon dubbed COVID-19, could only be countered, we were told, through the mobilization of a worldwide campaign to inoculate the entire global population.
On the way to the espoused goal of universal injections, humanity was subjected to absolutely nonsensical lockdowns at the local, national and global levels. The spread of this commercial madness crashed the world’s economy in ways that were planned. All the main elements of this preconceived devastation were totally unprecedented in global history.
We have yet to be presented with a credible explanation by the authorities responsible for what was and what is really going on. Why did all the measures that were supposed to help us, end up so severely harming us or even killing many victims? Why are the numerous deaths and injuries from the injections still being covered up? Who bears responsibility for the devastation caused?
The incarceration of Reiner Fuellmich symbolizes the intensity of the effort to prevent the truth of the whole matter from coming out.
The necessary international investigation should start with much-needed probs into the WHO. This UN agency is deeply implicated in what Reiner Fuellmich, the now-jailed and tortured German jurist, clearly described even during the early phases of the COVID debacle, as an elaborate complex of Crimes Against Humanity.
Anyone who has conscientiously followed the Covidian debacle from its inception will be aware of the hundreds of televised fact-finding interviews conducted by Fuellmich and his colleagues. He consulted hundreds of professionals with vital expertise that put them in a position to expose various aspects of the ongoing plague of disinformation coming from officialdom and their media spin doctors.
Already by September of 2021, the legendary lawyer made the following interim report of his findings. At that point Feullmich and his colleagues in the Corona Investigative Committee were just warming up in their intensive and extensive evidence-gathering initiative.
https://odysee.com/@GrandJury:f/Grand-Jury-1-EN:0
Before Fuellmich was able to initiate his well-conceived plan for an international legal procedure to address the well-orchestrated character of the COVID crimes, the legendary German jurist was kidnapped in Mexico and taken to Germany to be isolated in prison to face trumped up charges.
https://www.globalresearch.ca/reiner-fuellmich-persecution-prison%E2%80%A8/5870070
The WHO bears a huge responsibility for forcing on humanity a litany of lies and actions, all of which created major harms without any genuine remedial effects whatsoever. The WHO and its associated agencies should be investigated by an objective international body of arbiters possessing subpoena powers.
The COVID crisis built on the experience gained in floating the invented environmental crisis of climate change. Like “the environment,” “public health” is being used to create a boundless jurisdictional realm for globalist grifters who use the UN and the WEF for their own personal and corporate advantage.
In this scenario Bill Gates played a role at the United Nations and in the WEF rather similar to that Maurice Strong in the final decades of the 20th Century. Gates’ back up crew especially in Geneva and Davos was helped along by the Rockefeller Dynasty with their old and deep heritage of collaboration with China especially in the medical field.
The supposed wonder drug remedy for COVID-19 had nothing to do with the quest to put a stop to the spread of a respiratory virus. Rather the mRNA/lipid nanoparticle injections were disseminated in the context of many experiments within the framework of a single all-encompassing experiment directed at the entire global population.
The object of this process is to alter the genetic character—- the genomes— of the human species as well as of individual human beings. The news is very clear that the modification of humans to coordinate with AI and robotization is expected to be one of the most lucrative and active areas of industrial activity in the remainder of the twenty-first century.
Unless this travesty is identified, explained and halted, humanity can expect continuing experiments in methods of depopulation and digitalized enslavement to continue.
How the Corrupt Shape Shifters Promote and Exploit Environmentalism
The origins and many extensions of the UN’s “sustainable development” policies have a checkered history. This history was largely shaped by the power of bankers combined with the oil company leviathans that emerged from the monopolistic cartel initially fashioned by John D. Rockefeller.
Like other plutocrats, the Rockefellers became masters of combining “philanthropy” with the enhancement of their business endeavours. Bill Gates replicated and adeptly exploited this same kind of merger of charity and wealth accumulation.
The agents of the enterprises that sought to mould the concept of “sustainable development” have engaged in considerable shape shifting. They have tried to maintain the profit margins of large transnational corporations while adapting to upsurges of genuine public concern about the deteriorating health of the natural world.
The shape shifters have deployed many forms of deception aimed at manipulating environmental concerns while serving the interests of the domineering class of ruling kleptocrats. The World Economic Forum can be seen as an important site for plutocratic corporatist wolves to disguise themselves in sheeps’ clothing.
The manipulation of the concept of “sustainable development” reached a high stage of development in the so-called “Earth Charter.” This Charter is said to have emerged from the UN’s Conference on Environment and Development (UNCED) held in Rio de Janeiro, Brazil, 3 to 14 June 1992. One of the co-authors of the Earth Charter was Mikhail Gorbachev, former Soviet President.

The Rio Summit is sometimes referred to as the Earth Summit that is credited as a source of the Earth Charter. Much of the PR packaging of the most well-funded branches of the environmental movement can be traced back to the behind-the-scene politics of this event.

The Rio Summit proved to be a pivotal episode providing the initial impetus for the lofty-sounding environmental rhetoric replicated at the WEF by the ton-load. Always, however, the environmental laws are interspersed with provisos that subtly call for the transformations in property law.

The promoted alterations are well calculated to increase the concentration of wealth under the control of the predominant few. Their large fortunes are to be increased by the further dispossession and enfeeblement of the many.
The phrase, “You will own nothing and you will be happy” epitomizes the strategy of dispossession through environmentalist sleights-of-hand embodying strategies that stretch from David Rockefeller to Maurice Strong to Al Gore to Justin Trudeau.
One of those who made a big splash at the Rio Summit was Severn Cullis-Suzuki, daughter of David Suzuki, a leading evangelist of what has now become the climate change religion. Severn is now Executive Director of the Vancouver-based environmentalist conglomerate, the Suzuki Foundation.

https://davidsuzuki.org/expert/severn-cullis-suzuki/
The Rio Conference gave rise to Agenda 21, a kind of environmental manifesto published by the United Nations in anticipation of the twenty-first century. This manifesto was instrumental in raising the alarm that climate change was caused by humans and that the warming of the atmosphere was cataclysmic. Agenda 21 began with the proposition that
“current lifestyles and consumption patterns of the affluent middle class – involving meat intake, use of fossil fuels, appliances, air-conditioning, and suburban housing – are not sustainable.”
https://activistpost.com/2019/02/green-new-deal-reveals-the-naked-truth-of-agenda-21.html
According to Agenda 21 and to the UN’s Agenda 2030, what is not sustainable must be decreased in scale and ultimately brought to an end.

The assertions introduced in Agenda 21 are part of the long list of sacrifices that continue to be put before the public in the name of achieving a more harmonious equilibrium with the rest of nature.
The major figure behind the Rio conference in 1992 was Maurice Strong. The 1992 conference represented an extension on a much more ambitious scale of Strong’s organization of the UN’s first conference of “environmentalism.” This pioneering event that took place in Stockholm in 1972.
Feeling his oats at Rio, Strong followed up the gathering in Brazil with assertive pronouncements in including in Agenda 21. Strong’s assertions put people on a journey that has delivered us Westerners to the place we inhabit now. In Canada and other countries people are being pushed to adopt electric cars and put aside cars with internal combustion engines.
People are being asked by the likes of Bill Gates and his friend Justin Trudeau, to put aside meat and become self-abnegating cricket eaters.
Like Henry Kissinger, Strong was a hand-picked operative advancing the globalist agenda of David Rockefeller. For more than half a century, David Rockeller was the world’s most high-profile and influential banker.
Banker David Rockefeller
For a time Rockefeller was front and centre in organizing the finances of the UN. Rockefeller’s Chase Manhattan Bank was also in a strategic position to provide financial services to many of the UN’s new member countries. Most of the nation states recognized in the UN’s General Assembly emerged from the decolonization of European Empires following the Second World War.
David Rockefeller’s central role in building the doomed World Trade Centre in Manhattan is a fitting symbol of the magnitude of his many projects that most prominently included his key role in opening up China to the selective exercise of American capitalism.
The UN Headquarters in Manhattan is situated on land contributed to the international organization by the Rockefellers, the dynastic family that became the closest approximation in America to something like European Royalty.
Maurice Strong Attached “Sustainable Development” to Globalist Governance Headquartered at the United Nations
Strong was a Canadian who died in China in 2015. Strong operated on the borders of many “public-private partnerships.” These phantom relationships provide the cover to disguise the genre of kleptocracy promoted by the likes of Bill Gates and Klaus Schwab. While Strong worked with some of the most famous capitalists in his time, he considered himself a socialist in spirit.
His Aunt, Anna Louise Strong, was a dedicated socialist who obtained a Ph.D. at the University of Chicago and wrote 30 books. She interviewed Mao Zedong in Beijing and became his good friend. Leon Trotsky asked her to teach him English and wrote a Forward for one of her books. Ms. Strong spent many years in both the Soviet Union and China.
When the Soviet Union and China became acrimonious, Ms. Strong sided with China where she lived the last years of her life as did her nephew Maurice. Anna Louise Strong became one of a small group of US interpreters who pictured to Communist world with empathy rather than with Cold War hysteria.
Her career was comparable in the scale of her influence to that of her nephew. Maurice Strong kept in touch with his aunt who may have exercised more influence on him that is generally appreciated.

https://en.wikipedia.org/wiki/Anna_Louise_Strong
Strong grew up poor in small-town Manitoba. In 1947 he connected through a mutual acquaintance with the banker, David Rockefeller. Rockefeller saw qualities in the young Canadian that he thought he could shape, direct and exploit. In the 1950s Strong developed with Rockefeller involvement successful enterprises in Canada’s fledgling oil province.

Strong’s commercial feats during the early days of the Alberta Oil Patch brought him to the attention of the Power Corporation in Montreal. Power Corporation has been a very politicized commercial entity that helped put Pierre Trudeau, Jean Chretien, Paul Martin and Brian Mulroney into the job of Canadian Prime Minister.
Strong briefly became President of Power Corporation where he hired a young Paul Martin. Then Strong left in 1966 to join the upper echelons of the United Nations where he gave precedence to developing environmental agencies. He mixed his role at the UN with the founding and leading of the Canadian government’s International Development Agency.
In the 1970s and 80s Strong became a founder and then director of the World Economic Forum. In the early days of the WEF, Strong developed the organization’s capacity to reflect and advance the vision of many billionaires concerning what the most well-funded part of the environmental movement should look like.
Klaus Schwab has acknowledged that Maurice Strong was one of his mentors.

Schwab’s other main mentor was Henry Kissinger who, like Strong, owed most of his prominence in government to David Rockefeller.
Among the roles assigned to Strong were CEO of Petro-Canada and of Ontario Hydro. Other appointments made him senior advisor to the World Bank, the World Business Council on Sustainable Development, the World Conservation Union, and the World Wildlife Fund. The long list of his business, environmentalist and globalist involvements is truly vast.
https://corbettreport.com/meet-maurice-strong-globalist-oiligarch-environmentalist/
https://en.wikipedia.org/wiki/Maurice_Strong
cjournal.ca/2022/03/a-darker-shade-of-green-whats-behind-the-inexorable-rise-of-environmentalism/
Strong’s forte was spinning and exploiting the ultruistic intentions of many genuine activists seeking ecological rejuvenation.

On behalf of his sponsors, Strong helped to redirect the creative energies of many millions of well-intentioned folks to serve the objectives entrusted to him by his powerful backers.
The key to this redirection of ultruism was to funnel public attention from the complexity of genuine ecological menaces into a singular irrational fixation on the industrial role of carbon in the climate change boondoggle.
The climate change hoax provided Strong with a necessary scapegoat to funnel some semblance of popular will into the project of building up the power and pretensions of the United Nations. Then as now, the UN was being pushed into prominence as the site of ascendant global governance, a project pushed forward at the expense of the limitations imposed on the sovereign jurisdictions of the world’s almost 200 countries.
Strong advanced the agenda of his backers through membership in the UN-sponsored Brundtland Commission that helped make the term “sustainable development” a household phrase. The Commission produced in 1987 the report, Our Common Future. This initiative built on earlier initiatives emerging from the Club of Rome founded in the 1968.
This Club brought together some of the world’s most powerful people. They included David Rockefeller and Maurice Strong. The goal was to establish “limits to growth,” in other words to put some breaks on the genuine excesses and to create fear and alarm making the public more easily subject to manipulation.


Some suspect that the real agenda was for the ruling class to put the onus on average people to save the day by cutting back and living on less. Alternatively the perks and privileges of great wealth would continue with less of a chance that dominant oligarchs would have to face the revolutionary wrath of popular uprisings.

Maurice Strong” The Creator, Fabricator and Proponent of Global Warming”
Ronda Wilson has dubbed Strong as “the man who invented climate change.”
https://expose-news.com/2022/08/28/maurice-strong-invented-climate-change/

Another historian described Strong as the “primary creator, fabricator, and proponent” of the “Global Warming Hoax.”
In his essay, ‘Myths, Lies, and Oil Wars,” William Engdahl made a similar observation, indicating
“Canadian Maurice Strong was one of the key early propagators of the scientifically unfounded theory that man-made emissions from transportation vehicles, coal plants and agriculture caused a dramatic and accelerating global temperature rise which threatens civilization, so-called Global Warming.”
https://gfocusmagazine.com/?p=3409&lang=en
Strong adeptly used his multi-faceted influence to build up Operation Climate Change. With this strategic initiative he helped enlarge and empower the unaccountable imperial bureaucracy of the United Nations. Strong himself was a primary example of an unelected UN official who exercised much more power than most of the top elected officials in the world.
In 1988 the chief founder and spin doctor of the UN’s environmental agencies appointed himself to create the Intergovernmental Panel on Climate Change. In future years the IPCC was often put forward as if it constituted an unimpeachable authority backing the veracity of the Strong’s climate change narrative.
Strong authored the IPCC’s original mission statement. The UN’s top environment official made sure to limit the IPCC’s frame of reference to exclude any study of natural processes affecting changes to atmospheric temperatures.

This whole field of supposed scientific research on global warming and climate change was rigged from the beginning. Under Strong’s direction the whole enterprise was designed to produce a powerful lobby of privileged office holders geared to oppose any challenges to predetermined positions.
Strong arranged it so the ICPP came equipped with a big and growing budget as well as the administrative capacity of supervisors to direct commissioned studies towards preconceived objectives.

At the national and international levels, the administrators of the ICPP were afforded unlimited discretion to select researchers so as to make sure the panel supported and advanced the predetermined conclusions. There is ample evidence of the machinations which erupted when ICPP contributors did not go along with the official narratives.
https://climatechangereconsidered.org/about-the-ipcc/
The demonization of carbon and especially of CO2 as the main menace to nature is a lie that in the long run is unsustainable. The notion of the monstrous impact of so-called greenhouse gases is also unsustainable. Water vapour is by far the main greenhouse gas.
The irony of characterizing plant food as the tip of the spear in the industrial assault on Mother Nature, must have appealed to Strong’s sense of humour.
https://greenmedinfo.com/content/demonization-co2-challenging-prevailing-narrative
To classify carbon, a main ingredient of all life on earth, as a enemy of life is strange to say the least. Yet somehow the theory of global warming took hold and there has been ample funding to maintain this wonkey theory as holy gospel ever since.
In spite of all the constraints contrived to block critical examination, independent researchers have popped up here and there to question the orthodoxy causing Dr. Tim Ball to explain “Why and How the IPCC Demonized CO2 with Manufactured Information.”
See also
https://wattsupwiththat.com/2018/07/07/whatever-happened-to-agenda-21-and-climate-change-policy/
https://principia-scientific.com/co2s-role-in-the-great-climate-change-deception/
The simplistic and badly distorted picture of the nature of the earth’s atmospheric environment was manipulated by Maurice Strong and others to make carbon removal through sequestration the driving force in the creation of a new type of currency.
This currency can facilitate a new form of commercial transaction that builds on the notion of “carbon offsets.” In these markets of plus and negative carbon, those engaged in industrial processes that emit carbon can purchase the “right” to continue emitting carbon without being fined. They can buy this “right” from those that have made a business of removing carbon from the atmosphere.

In the end, the supposed polluters pay fiat dollars for credits from carbon eliminators. The carbon eliminators earn CERs, “Certified Emission Reductions,” that they can sell to those seeking to avoid being penalized for the supposed environmental crime of releasing CO2 into the atmosphere.
This whole structure of economic relations has given rise to the notion of a tax even on average people deemed to be polluters for, say, heating their homes in a Canadian winter, or driving to the store to buy food and medicine, or running computers to work at home.

There are few or no penalties for industrial enterprises that release many toxic chemicals not given celebrity status like carbon. All companies have to do to get a clean bill of environmental health is to enter the process of buying carbon emission rights from those that sell CERS.

The UN apparently cannot intervene to stop genocide in Gaza where people are murdered en masse in the midst of environmental desecration on a monumental scale. But the UN can apparently attract many businesses into its system for engaging them in useless, energy wasting procedures in the effort to balance carbon emissions with carbon capture.
The UN can create the theatrics, if not the substance, of environmental justice. Simultaneously UN officials watch on while the provision of the UN Charter are systematically violated through unregulated war mongering that is cancelling all prospects of peace.
While the world lurches towards the prospect of nuclear oblivion, the UN is fiddling with carbon flows with the aim of achieving etherial equilibrium through some sort of “netzero” nirvana.

In 2007 in an essay entitled “Carbon Trading,” Strong lauded
“the use of market mechanisms to mobilize funding for clean energy projects, reduction of carbon dioxide and other greenhouse gas emissions on a cost-effective basis through the Clean Development Mechanism (COM), and the trading of Certified Emission Reductions (CERs), provided for by the Kyoto Protocol to the United Nations Framework Convention on Climate Change.
https://www.mauricestrong.net/index.php?option=com_content&view=article&id=190&Itemid=101
One of Strong’s main messages is that China, where he permanently lived in 2007, was adopting the system for purchasing and selling carbon credits. The Communist Party of China was adding its enormous weight of influence to the creation of a new form of currency initially floated at the United Nations as part of Maurice Strong’s Climate Change Empire.
The buying and selling of carbon-related chips anticipated the proliferation of many new forms of exchange unfolding in the present era. Currently many new forms of cryptocurrencies are vying for legitimacy against the weakening power of the rapidly-inflating US dollar supply.
Strong moved to China after being caught with a million dollar cheque that was said to be part of a bribe related to the Food for Oil scandal in Iraq. The scandal involved kickbacks to the government of Saddam Hussein. In 2005 the CBC reported
“In an indictment that was unsealed Friday, U.S. prosecutors said Park received millions from the Iraqi government to bribe UN officials in a scheme to undermine the oil-for-food program
https://www.cbc.ca/news/world/strong-denies-part-in-un-oil-for-food-scandal-1.540516
https://www.fdd.org/analysis/2007/02/06/at-the-united-nations-the-curious-career-of-maurice-strong/
Rather than face the scandal, Maurice Strong moved to China. Over the course of his life, Strong, like his patron David Rockefeller, would travel to China frequently. Strong would sometimes visit his Communist Aunt who apparently had “befriended” both Lenin and Trotsky when she was living in Russia.
https://corbettreport.com/meet-maurice-strong-globalist-oiligarch-environmentalist/
Is it possible that, among his many commitments, Strong was an agent involved in the affairs of the Chinese government. Among these affairs could well have been China’s important interactions with David Rockefeller. Throughout the 1970s Strong’s mentor, the UN’s banker, often travelled to China where he is known to have travelled extensively throughout the country by train.
The Rockefellers are known to have been Sinophiles raised in a home adorned with Chinese finery. Going back to the nineteenth century, John D. Rockefeller was actively engaged in selling kerosene in China. In the early twentieth century, the Rockefellers directed their attention to running of a hospital in China and in assisting with the establishment of Higher Education.
By 1973 David Rockefeller travelled to China and met Zhou Enlai as a prelude to opening up banking interactions that proved to be instrumental in radically transforming the nature of US-Chinese relations.

Whatever the motivation, Strong too was a Sinophile who opted to spend his final years in China.
Mao Tse Tung was close to Maurice Strong’s Aunt, Anne Louise Strong
Geo-Engineering, Environment, Ecology, and Bio-Weapon Attacks
There is no doubt that the natural world has and is being harmed by many forms of industrial activity, much of it focusing in and around military conflicts. A major category of atmospheric interference has been categorized as geo-engineering, much of it conducted secretly by branches of the world’s many Armed Forces. See
Carbon is Not the Enemy. End Chemtrails!
Aug 29
Read full story Back to Text
For governments to ignore the effects of geo-engineering on nature, including on human settlements, is highly disingenuous. It is especially unforgivable for governments to hide abundant evidence of geo-engineering while diverting so much public attention to a very flawed account of anthropogenic [human caused] climate change.
https://www.globalresearch.ca/climate-change-and-geoengineering/1120
https://www.geoengineeringwatch.org/geoengineering-weather-warfare-and-the-contrail-deception/
The extremely volatile and unusual character of the Maui fires in the summer of 2023 offers one prominent example among many which indicate that military agencies are deeply engaged in dramatic alterations of atmospheric conditions with the goal of doing devastating and highly-targeted harm.
Much has changed since Maurice Strong came up with his theory of climate change that coincided so well with his agenda of building up the role and the reach of the United Nations. Strong took further the ideas introduced by the Club of Rome and the Brundtland Commission.

The essence of their findings was that public fears about environmental degradation could be effectively manipulated to scare people into compliance with directives emanating from governments, industry, and high finance.

Putting aside the phenomenon of psychological warfare through engineered fears of devastating climate change, some of the thinking generated by independent voices within the environmental movement have contributed important understandings. A large theme of the revelations has been the importance of looking deeply into the thick web of biological interactions among diverse plants and animal as emphasized in the scientific study of ecology.
This study has contributed to the crucial understanding that the health of people is intimately connected to the health of the larger community of life forms with whom we share the planet. The understanding of intertwined biological interactions of the many millions of organisms throughout nature generally, can also be pointed inwards.
We edify ourselves when we recognize the unique complexity of the many facets of our own inner selves, physically, spiritually, and intellectually. We must come to know ourselves in order to be true to ourselves. Humanity cannot thrive in collectivities or as individuals when we are all made subject to one-size-fits-all dictates as epitomized by the push to universally inject the global population with gene-modifying concoctions.
It is time to address the UN’s recruitment of the word, “environment” as an open-ended term ideal for staking out broad jurisdictional turf in a global context. There are many kinds of environments, including, for instance, mental environments, cultural environments, cosmic environments, economic environments, political environments and so on.
The destruction of natural environments is often accompanied by the destruction of mental environments in ways that make reasonable public discourse impossible. Rational public debate, on which much depends, becomes nearly impossible when the mental environment becomes toxic. Pollution of thought flows from pollution of the mental environment.
Atmospheric cycles of change sometimes referred to as “the weather,” do not conform to geopolitical boundaries. Accordingly the use of the term, “the environment,” can be seen as a word choice well calculated to accommodate the expansion of global governance centred at the UN.
Clearly Bill Gates and his backers in the Rockefeller Foundation have come to similar conclusions by highlighting “public health” as a means of transcending boundaries in the governance of people worldwide. Gates became a major funder of the UN’s World Health Organization whose leadership continues to push for new powers to negate the national sovereignty of member countries.
Because of such developments, Parliaments and Legislatures everywhere are coming to seem more and more like museums. These remnants of a bygone era remind many average people of the time when we used to have at least a chance of exercising some influence in determining the actions of our own governments.
Rather than being places of self-governance for we the people, our legislative buildings are becoming places where accumulations of rubber stamps give the appearance, without the substance, of legitimacy to many transaction. The rubber stamps contain edicts that come about through rigged elections, rigged media reports, rigged search engines, rigged court procedures combined with the rigged ascendance of proliferating globalist institutions.
The United Nations and its partner, the WEF, have become emblematic of globalist governance by, for, and of the plutocrats. As the world’s primary international organization, the UN is certainly a reflection of internationalism gone astray. Internationalism points away from national sovereignty towards a more Marxian emphasis on conflict between haves and have nots.
As a self-identifying socialist internationalist, Maurice Strong saw the world through the prism of class conflict within countries. This dynamic of material conflict over access to natural resources extended to antagonisms between rich and poor regions. Some view the climate change hoax set in motion by Maurice Strong as a scheme whose real objective was the redistribution of wealth.
The WHO’s oversight of the broad outlines of the globalist bioweapon attack done in the name of vanquishing COVID-19, drew on a hypothetical scenario provided in a report of the Rockefeller Foundation in 2010. The predictive document was in the chapter, “Lock Step.” This chapter” is part of a report entitled, Scenarios for the Future of Technology and International Development.

https://www.nommeraadio.ee/meedia/pdf/RRS/Rockefeller%20Foundation.pdf
Those behind the scheme to inject every person on the planet with injected, gene-altering bioweapons are still at large among us. The appreciation of the sanctity of human life has always been partial and problematic but now the gloves are off and the truth is out in the age-old battles for survival.
Looking out at the World from Canada is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.






















")














{kind=link}
ReplyHENRY DE LESQUEN
38.3K subscribers
Cette vidéo a été réalisée le 11 mars 2020, la veille de la première allocution solennelle de Macron sur le coronavirus. Depuis, le professeur François Bricaire, infectiologue, membre de l'académie de médecine, a confirmé les conclusions rassurantes du professeur Didier Raoult que nous avions citées : le covid-2019 n'a rien d'exceptionnellement dangereux. Le confinement imposé par Macron est donc une mesure excessive, disproportionnée, irrationnelle, aberrante, économiquement désastreuse et, de surcroît, liberticide, puisqu'elle porte atteinte à la liberté d'aller et de venir, liberté essentielle s'il en est. C'est une décision extravagante, improvisée dans un climat de panique, qui va à l'encontre d'une analyse objective des coûts et des avantages de cet assujettissement exorbitant des Français à l'Etat.
Blaming Bill Gates, Dr. Fauci, WHO, the UN AGENDA 21, NASA, 5G, HAARP, CHEMTRAILS, BIG PHARMA, ETC. IS UTTERLY USELESS BECAUSE THE STATE IS THE MAIN CULPRIT AND THERE IS NO COURT SYSTEM TO TAKE ANYONE OF THEM TO BE PROSECUTED AND CONVICTED AND NO AXE, NO GUILLOTINE, NO HOMICIDAL GAS CHAMBER, NO HANGING ROPE AND NO FIRING SQUAD TO EXECUTE THEM AS THEY DO NOT DESERVE TO LIVE, NOT EVEN ONE DAY!
ALL WE DO IS TALK, TALK, TALK, AND NO ACTION!
AND, THE STATE KNOWS WE ARE STUPID! SO THEY ALWAYS GO AHEAD AS PLANNED!
THEY HAVE NEVER HEARD THE ABOUT THE BEST WEAPON WE HAVE TO STOP THEM: TOTAL CIVIL DISOBEDIENCE, TOTAL ECONOMIC, MEDICINAL, GMO AGRICULTURAL, EDUCATIONAL, SCIENTIFIC, MEDIA, TELEVISION, CINEMA, SPORTS, AND CULTURAL BOYCOTT, AND RETURN ALL POWER TO THE PEOPLE.
LESS THAN THAT, WE ARE HEADING STRAIGHT TO HELL!
BAFS
FRIDAY 1ST OF MAY 2020
“THEY” HACKED MY BLOG, REMOVED MY PERSONAL PHOTOS AND COLLAGES, BLOCKED ME TWICE ALREADY ON FACEBOOK BECAUSE OF THIS STUPID-19 (Mike King) STATE AND MEDIA PSEUDO PANDEMIC NON CRISIS PSYCHOSIS “PROPAGANDA MASQUERADING AS SCIENCE” (Dr Judy A Mikovits PHD)– ACCUSING ME OF HATE SPEECH, RACISM, PROMOTING DANGEROUS CHARACTERS, ETC.
THIS POST HACKED AND MORE THAN SIX PERSONAL PHOTOS OF CHEMTRAILS, EMPTY SHELVES IN SUPERMARKETS, ETC. REMOVED???
ReplyTHE MESSAGE IS CLEAR - DON'T POST AGAIN!!!
BAFS
23/04/2020
Now, Facebook has DE-ACTIVATED me without warning! Most probably for this latest post:
ReplyMUHAMMAD ALI BEN MARCUS
Tuesday, 1 September 2020
ACHTUNG! THAT SHITTY GOVERNMENT AND ITS SEWAGE SCHOOL SYSTEM TAKING OUR KIDS HOSTAGE !
https://muhammad-ali-ben-marcus.blogspot.com/2020/09/achtung-that-shitty-government-and-its.html
Émergences-Formations - ANNONCE - « Officiel : il n'y a jamais eu de pandémie en 2020 »
ReplyTHERE WAS NEVER ANY PANDEMIC IN 2020!
Émergences-Formations
To:bafremauxsoormally
Mon, 26 Oct at 02:21
Bonjour BASHEER FRÉMAUX-SOORMALLY,
Il y a une nouvelle annonce pour le bloc de formation « CHAÎNE PRIVÉE GRATUITE DE JJC ! » :
Voici le contenu de cette annonce ;
Bonjour,
Non, tu ne rêves pas. J'affirme (et je prouve) dans ma nouvelle conversation du lundi qu'il n'y a jamais eu de pandémie en 2020.
J'en fais la démonstration pour la France dans la CDL61 intitulée - Nourrir la vision du futur et désobéir en actes que tu peux visionner en cliquant ici !
Et je prépare la même démonstration pour la Belgique, la Suisse et le Québec…
J'espère avoir suffisamment attisé ta curiosité pour te donner l'envie d'aller faire un tour sur la chaîne privée.
Et surtout : ne perds pas courage. Les gouvernements multiplient les provocations en imposant des mesures de plus en plus injustifiées et injustifiables. La fin des mensonges et des manipulations est proche !
Alors, gardons dans nos cœurs ce futur auquel nous sommes des millions à aspirer. Et manifestons à travers nos actes de désobéissance que nous ne leur donnons plus le pouvoir de nous soumettre…
Jean-Jacques
PS : Merci de n’écrire au support clientèle QUE si tu as besoin d'une aide technique ou administrative.
=> Pour déposer des documents ou des informations : https://documents.apaga.net
=> Merci encore une fois à ceux et celles qui chaque semaine rejoignent les abonnés qui souscrivent un abonnement de soutien volontaire… C'est très très précieux pour nous et ça nous permet de continuer à nous concentrer sur cette démarche de défense de nos libertés et de nos droits fondamentaux…
=> Si toi aussi, tu veux soutenir notre action, clique sur ce lien : https://formations.emergences.net/chaine-abonnement-ps
=> Pour accéder à la chaîne privée : https://formations.emergences.net/login
=> Pour permettre à quelqu’un de s’inscrire à cette chaîne privée : https://formations.emergences.net/iln0002-chaineprivee
=> Pour te désinscrire de la chaîne, annuler un abonnement payant ou mettre à jour tes préférences : https://formations.emergences.net/iln0002-desabonnement
Pour te connecter à ton compte, clique sur le lien ci-dessous:
https://formations.emergences.net/login
Émergences-Formations.
Tom Woods
ReplyTo:bafremauxsoormally
Fri, 30 Oct at 15:49
Remember that creep Dr. Zeke Emanuel?
I'll refresh your memory:
"We cannot return to normal until there's a vaccine. Conferences, concerts, sporting events, religious services, dinner in a restaurant, none of that will resume until we find a vaccine, a treatment, or a cure....
"We need to prepare ourselves for this to last 18 months or so and for the toll that it will take. We need to develop a long-term solution based on those facts. It has to account for what we are losing while this fight goes on, things like schooling and income and contact with our friends and extended family."
He wanted you to go for 18 months without "schooling and income and contact with [your] friends and extended family."
Dr. Emanuel is advising Joe Biden on the virus.
If you're curious about what he would advise Joe to do, here's what he said back when he thought Italy had "crushed the curve" (with thanks to Alex Berenson):
"One of the important things for all your readers to look at is Italy.
"Italy did a nationwide lockdown.... We’ve never gotten as low as Italy is today.... We needed that kind of process nationwide, and we did not have that.
"So that’s one thing: a nationwide lockdown that lasts 8 weeks until we have a number of new cases in the 2 to 3 per 100,000 level."
He said this in September.
Italy just reported 217 deaths from the virus yesterday, which is the equivalent of 1200 deaths in the U.S.
Gee, Dr. Emanuel, it looks like locking people in their houses only delays the inevitable -- as everyone at the time tried to tell you.
Tom Woods
ReplyDr. Rashid Buttar The Real Battle Is Not The Virus: How the Coronavirus Agenda is Eroding Our Civil Liberties
3,005 views •
October 30, 2020
Making his third appearance on the Digital Freedom Platform, Dr. Rashid Buttar is an American doctor and author with over 30 years experience in the medical field.
Dr. Buttar has been ranked in the ‘Top 50 Doctors in the US’ since 2003, and released his first book called; “The 9 Steps to Keep The Doctor Away”, which became a Wall Street Journal, USA Today and Amazon bestseller.
Yet despite his experience, Dr. Rashid Buttar has been marked as “the most censored doctor in the world”, and has been subject to banning and shadow banning across social media platforms.
It’s not something that has gone unnoticed by Dr. Buttar who has commented: “I had 413,000 subscribers and in three days I had 84,000 new subscribers – that was nine weeks ago, since then I haven’t had one single new subscriber.”
He returns to the Digital Freedom Platform today to outline the next phase of the COVID-19 agenda and expose government measures already in place.
The UK is now in separate lockdowns ranging from Tier 1 to Tier 3, and it seems there has been a lack of leadership and science-based decisions when tackling this pandemic.
Dr. Rashid Buttar believes a further erosion of civil liberties will be continued leading into 2021.
Join us on the Digital Freedom Platform as we discuss censorship, the Coronavirus agenda and what lies ahead for 2020 and beyond.
https://freedomplatform.tv/dr-rashid-buttar-the-real-battle-is-not-the-virus-how-the-coronavirus-agenda-is-eroding-our-civil-liberties/?vgo_ee=Bp9Ps0udyyq8JO5PjoBtynEK5gmiTKnqE2cylyNoeqk%3D
ReplyROSE/BUTTAR III
The Real Battle Is Not The Virus
Hi Basheer,
As the world keeps turning, as do the wheels of change to our daily lives and routines. As the powers that be muddle through the latest roll out of lockdown restrictions and protocols, the world sits by anxiously waiting, wondering, whispering - what is coming next?
Today’s guest, Dr Rashid Buttar, is making his third appearance on the Digital Freedom Platform and this interview couldn’t be more timely. Dr Buttar has found himself front and centre of the information war that has been raging during the hostile months that have surrounded the global lockdown.
Dubbed ‘the most censored doctor on the planet’, Dr Buttar, who has been working in the medical field for over 30 years and regularly found his name ranked as one of the ‘top 50’ doctors in the US, has seen his resolve tested through his determination to ensure every man, woman and child has access to information regarding the COVID agenda and the fundamental characteristics of human nature.
His forthright approach has seen him silenced, shadow banned and oftentimes erased by the major tech companies operating as both judge and jury in what is rapidly becoming a digital wild west.
How The Coronavirus Agenda Is Eroding Our Civil Liberties
With so much still to understand about the Coronavirus outbreak and the seemingly contradictory and confusing policy responses from our leaders, it’s little wonder we now face a mental health epidemic to accompany our supposedly fractious physical well being.
Let me be clear: this is important information that corresponds directly to much of the narrative we see unfolding across the globe.
From the biological realities about immune systems and its hard wired capabilities, to the vaccine agenda and the pre-planned objectives for the months ahead, to a leaked email from the Canadian Liberal Party that if true will change the lives and prosperity of many indefinitely, Dr Buttar speaks with authenticity and clarity on a range of the most pressing issues we face.
An intelligent, passionate and hardworking family man, who has dedicated his life to helping others, I encourage you to join Dr Buttar and myself for this revealing conversation. Don’t miss this opportunity to get a better understanding of what is happening in our world, so you can make a personal and informed opinion from a broad range of views.
Make sure you don’t miss this episode live and exclusive on our Digital Freedom Platform and share the link with all like minded friends and family.
© Crown copyright
ReplySkip to main content
GOV.UK
Search on GOV.UK
https://www.gov.uk/guidance/high-consequence-infectious-diseases-hcid#status-of-covid-19
Status of COVID-19
As of 19 March 2020, COVID-19 is no longer considered to be a high consequence infectious disease (HCID) in the UK.
The 4 nations public health HCID group made an interim recommendation in January 2020 to classify COVID-19 as an HCID. This was based on consideration of the UK HCID criteria about the virus and the disease with information available during the early stages of the outbreak. Now that more is known about COVID-19, the public health bodies in the UK have reviewed the most up to date information about COVID-19 against the UK HCID criteria. They have determined that several features have now changed; in particular, more information is available about mortality rates (low overall), and there is now greater clinical awareness and a specific and sensitive laboratory test, the availability of which continues to increase.
The Advisory Committee on Dangerous Pathogens (ACDP) is also of the opinion that COVID-19 should no longer be classified as an HCID.
100,000 UK Covid deaths: the highest in Europe - BBC News
Reply41,861 views
•26 Jan 2021
BBC News
9.15M subscribers
The United Kingdom is the first European country to record more than 100,000 deaths linked to the pandemic.
According to the University of Oxford the UK has one of the highest Covid death rates anywhere in the world.
The prime minister Boris Johnson, whose handling of the pandemic has been heavily criticised by some people, said he was “deeply sorry for every life lost” and took “full responsibility for everything that the government has done”.
Almost 250,000 people have been admitted to hospital with Covid since the start of the pandemic.
Professor Chris Whitty, the UK's chief medical adviser, said there would be many more deaths in the coming weeks.
Huw Edwards presents BBC News at Ten reporting by health correspondent Catherine Burns, political editor Laura Kuenssberg, and health editor Hugh Pym.
N.B. IMMEDIATELY AFTER I HAD POSTED SOME 10 SNIPPETS FROM THE ABOVE POST, AT 3AM, 27.1.2021, ALL BUT ONE HAVE VANISHED??? WOW!
BAFS
The above posted Youtube video by Brendon Lee O'connell was removed by Youtube:
Reply"This account has been terminated due to multiple or severe violations of YouTube's policy prohibiting hate speech."
Nygard, Maxwell and Epstein: Charlie Robinson
Reply•12 Apr 2021
https://www.youtube.com/watch?v=ASNqU6kO5-w
Shaun Attwood
666K subscribers
Charlie Robinson's Macroaggressions Podcast: https://podcasts.apple.com/us/podcast... Charlie's book: https://books2read.com/u/b6OR6y Website: http://theoctopusofglobalcontrol.com/ Our Patreon tiers: https://www.patreon.com/shaunattwood?... Watch the Unleashed Series: https://www.youtube.com/playlist?list... Watch 400+ Epstein videos: https://www.youtube.com/playlist?list... Maria Farmer on Twitter: https://twitter.com/ArtisticBlower Virginia Roberts on Twitter: https://twitter.com/VRSVirginia Annie Farmer on Twitter: https://twitter.com/anniefarmer
DR. VERNON.COM
ReplyI'm Losing Patience with the Zombies
https://brandnewtube.com/watch/i-039-m-losing-patience-with-the-zombies_XqoCT4bfyK3XkJ7.html
In recent months, Dr Coleman's videos have been heavily targeted by paid trolls spreading lies and libels about him, which is why he has had to disable comments. Dr Coleman apologises and hopes that you understand.
To buy Dr Coleman's latest book called, 'Endgame - The Hidden Agenda-21' click here https://www.amazon.co.uk/Endga....me-Hidden-Agenda-Ver
For more unbiased information about other important matters, please visit https://www.vernoncoleman.org
COVID-19 OFFICIALLY DOWNGRADED TO FLU ON 19 MARCH 2020!!!
BILL GATES, THE CROWN, CORPORATIONS, AND GOVERNMENTS BEHIND THE CORONA SARS COV2 COVID19 VIRUS SCARE!
Replyhttps://muhammad-ali-ben-marcus.blogspot.com/2020/03/bill-gates-crown-corporations-and.html
My Blog was attacked as soon as I posted the above on Thursday, 19 March 2020, and my Facebook page was blocked and terminated in early September 2020!
I had found hard and indisputable evidence of the pandemic hoax, a WHO-GATES-FAUCI-BUZYN FORT DIETRIC-PASTEUR-WUHAN PLANDEMIC, and also that Trump had signed HR-748 CARES ACT on 27 March 2020, that Congress had introduced more than a year before on 24 JAN 2019, but most of us do not give a damn!
US Congress CARES Act = CORONAVIRUS, AID, RELIEF, and ECONOMIC SECURITY Act INTRODUCED ON 24 January 2019???
21 videos posted not available anymore???????
ReplyCRYPTO-JEW JESUIT OATH (ANTHONY FAUCI)
ReplyQuestion —From whither do you come? Answer — The Holy faith.
Q. —Whom do you serve?
A. —The Holy Father at Rome, the Pope, and the Roman Catholic Church Universal
throughout the world.
Q. —Who commands you?
A. —The Successor of St. Ignatius Loyola, the founder of the Society of Jesus or the Soldiers
of Jesus Christ.
Q. —Who received you? A. —A venerable man in white hair.
Q. —How?
A. —With a naked dagger, I kneeling upon the cross beneath the banners of the Pope and of
our sacred order.
Q. —Did you take an oath?
A. —I did, to destroy heretics and their governments and rulers, and to spare neither age, sex
nor condition. To be as a corpse without any opinion or will of my own, but to implicitly
obey my Superiors in all things without hesitation of murmuring.
Q. —Will you do that? A. —I will.
Q. —How do you travel? A. —In the bark of Peter the fisherman.
Q. —Whither do you travel? A. —To the four quarters of the globe.
Q. —For what purpose?
A. —To obey the orders of my general and Superiors and execute the will of the Pope and
faithfully fulfill the conditions of my oaths.
Q. —Go ye, then, into all the world and take possession of all lands in the name of the Pope.
He who will not accept him as the Vicar of Jesus and his Vice-regent on earth, let him be
accursed and exterminated."
VITAL! The Italian Boss of Obama’s Coronavirus. Ukraine Laboratories Funded by former CIA Director Leon Panetta
Reply1 – PANETTA, SPEARHEAD OF OBAMA AND DEEP STATE
2 – YOUNG SON OF CALABRIANS IN MILITARY INTELLIGENCE
3 – 2004, THE BEGINNING OF THE ORWELLIAN PLAN: WUHAN-CIA
4 – GATES IMMUNIZATION PLAN AND CORONAVIRUS HUNTING
5 – PANETTA: FROM THE CIA TO THE PENTAGON IN THE AGE OF CHIMERIC VIRUSES
6 – A FLOOD OF DOLLARS FROM THE PENTAGON TO UKRAINE
7 – FROM CORONAVIRUS TO BIG PHARMA VACCINES: ITALY-US DEM PLAN
https://www.vtforeignpolicy.com/2023/05/vital-the-italian-boss-of-obamas-coronavirus-ukraine-laboratories-funded-by-former-cia-director-leon-panetta/
ReplyZuckerberg Confession: “Establishment asked Facebook to ‘censor’ Covid posts”
By
Fabio G. C. Carisio -
June 11, 2023
https://www.vtforeignpolicy.com/2023/06/zuckerberg-confession-establishment-asked-facebook-to-censor-covid-posts/
Facebook was asked by the scientific “establishment” to remove various posts related to Covid-19 which later proved to be “debatable or true,” Meta CEO Mark Zuckerberg said during a podcast interview this week.
Speaking to the Russian-American interviewer Lex Fridman in a podcast released on Thursday, Zuckerberg said that policing Facebook’s attempts to remove mistruths is “really tricky.”
“Just take some of the stuff around Covid earlier on in the pandemic,” Zuckerberg explained, “Where there were real health implications but there hadn’t been time to fully vet a bunch of the scientific assumptions.”
“COVID mRNA VACCINES ARE LIKE GENE THERAPIES”. French Biologist's Study Denounces Omitted EMA Controls on Genotoxicity
Replyhttps://www.gospanews.net/2023/07/13/i-vaccini-covid-mrna-sono-terapie-geniche-studio-francese-revisionato-denuncia-gli-omessi-controlli-ema-sulla-genotossicita/?unapproved=28653&moderation-hash=71259fd5b7c52ee0879cda203f219a9d#comment-28653
It is not for the Common people to get involved in scientific and pseudo-scientific bickering. All the Common people needed to know was whether the PANDEMIC was real or fake, planned and staged for reasons that would not solve the problem, but make the Deadly Big Pharma richer, and allow the Government to lock down the country, killing the most vulnerable among us and traumatise an entire nation, and in particular the small ones that State and Media Terrorism were attacking as well, and cut down on Health Care and Social Services. The Common people needed to know whether the so-called vaccine was the solution to successfully neutralise the cause of the Pandemic for which we already have all the evidence necessary that it was planned well in advance.
I just saw that even Hélène Banoun playing up, and minimising the seriousness of that deadly experimental Big Pharmaco-Biotechncal Engineered MESSENGER DNA (mRNA) Weapon destined to be used against 8 billion people worldwide, except the Élite, obviously.
“COVID-19 vaccines were developed and approved rapidly in response to the urgency created by the pandemic. At the time of their marketing there were no specific regulations. Regulatory agencies therefore adapted them as a matter of urgency. With the pandemic over, it's time to consider the safety issues associated with this speedy approval. The mode of action of COVID-19 mRNA vaccines should have classified them as gene therapy products (GTPs), but they have been barred by regulatory agencies. Some of the tests they have been subjected to as vaccines have produced non-compliant results in terms of purity, quality and homogeneity of the batches ».
THIS IS NOT SCIENCE: "developed and approved rapidly":???
The scientifically UNPROVEN PANDEMIC where ZERO VIRUS WAS ISOLATED created an "urgency"? This is State BS, not SCIENCE!
"With the pandemic over"? Which pandemic? When? Where? Kary Mullis was murdered in 2019 for saying the test he invented could not be used to diagnose any infection! Dr. Rashid Buttar was murdered for saying the pandemic was planned long in advance, which it was, and the vaccines were bogus and deadly, which they proved to be!
It was not SCIENCE that decided the " experimental Big Pharmaco-Biotechncal Engineered MESSENGER DNA (mRNA) Weapon" was not a Gene Therapy Product, but the profiting manufacturers with their State and W.H.O.'s accomplices.
BAFS
Former Head of Biology (1970s)
Trinity Colleges (Mauritius)
MUHAMMAD ALI BEN MARCUS
Thursday, 19 March 2020
BILL GATES, THE CROWN, CORPORATIONS, AND GOVERNMENTS BEHIND THE CORONA SARS COV2 COVID19 VIRUS SCARE!
https://muhammad-ali-ben-marcus.blogspot.com/2020/03/bill-gates-crown-corporations-and.html
https://www.gospanews.net/2023/07/13/i-vaccini-covid-mrna-sono-terapie-geniche-studio-francese-revisionato-denuncia-gli-omessi-controlli-ema-sulla-genotossicita/
ReplyFranck Unsubscribe
ReplyTo:bafremauxsoormally
Mon, 14 Aug 2023 at 07:00
CHER FRANCK
Merci, mais il n’y a jamais eu de COVID-19 en dehors de la grippe saisonnière ! Et, il n’y a aucun vaccin hormis des armes meurtrières bio-tech, stérilisatrices, et qui dégénèrent notre espèce humaine ! Des scientifiques tels Kary Mullis, et des médecins pratiquants et braves tels Claire Séverac, Rashid Buttar, et d’autres furent assassinés pour avoir osé s’opposer aux mensonges des oligarques à qui cela profite – principalement la Cabale eugéniste.
La médecine naturelle existe depuis la nuit des temps ainsi que le savoir vivre pour soulager et guérir toutes les maladies. Alors, pourquoi promouvoir des produits pharmaceutiques (sataniques) des mêmes oligarques et à des coûts aussi exorbitants ?
Cordialement
BASHEER
Ce lundi 14 août 2023
MUHAMMAD ALI BEN MARCUS
Thursday, 19 March 2020
BILL GATES, THE CROWN, CORPORATIONS, AND GOVERNMENTS BEHIND THE CORONA SARS COV2 COVID19 VIRUS SCARE!
https://muhammad-ali-ben-marcus.blogspot.com/2020/03/bill-gates-crown-corporations-and.html
MIKE ADAMS - COVENOM-19
ReplyPart 1/3 - Dr. Bryan Ardis reveals BOMBSHELL origins of covid, mRNA vaccines and treatments
https://www.brighteon.com/2b090826-787f-4d03-9f78-a1a80d3fe767
Part 2/3 - Dr. Bryan Ardis reveals BOMBSHELL origins of covid, mRNA vaccines and treatments
https://www.brighteon.com/a91f6ff5-b39d-49bc-9619-4c148335a5b3
PART 3/3 - DR. BRYAN ARDIS REVEALS BOMBSHELL ORIGINS OF COVID, MRNA VACCINES AND TREATMENTS
https://www.brighteon.com/7aa69398-89bd-497e-a075-cc9b96176bef